(ambiguous genitalia, sexual ambiguity)
The terms hermaphrodism (hermaphroditism) and intersex are no longer used.
Embryological reminder :
The human embryo has the dual potential to develop its genital tracts as a male or female phenotype. The presence of the SRY gene on the short arm of the Y chromosome directs the differentiation of the gonad in the direction of a testicle that will secrete 2 hormones:
- the anti-mullerian hormone (Sertoli's cells), causing the regression of the Muller's canals;
- the testosterone (Leydig's cells) allowing the development of the Wolff's canals: its active derivative, dihydrotestosterone, attaches to the receptors responsible for the virilization of the external genitalia and the urogenital sinus.
In the absence of the SRY gene (see Swyer syndrome), the gonad differentiates as an ovary and the Muller's canals persist; they will form the fallopian tubes at their cranial extremity and, by merging their caudal extremity, the uterus and the upper part of the vagina.
Diagnosis approach in the neonatal period :
Sexual ambiguity results from an abnormality in the differentiation of the external genitalia or from a discordance between the external and internal genitalia. It is rare (but still possible nowadays) that the diagnosis is only made at puberty or even in adulthood in the presence of heterosexual puberty or primary amenorrhea (feminizing testicle).
Ambiguity is usually recognized in the neonatal period. The diagnosis is evident at birth in major forms, but it can be difficult in less obvious forms: micropenis with bent penis (actually corresponding to a clitoris), clitoral hypertrophy, cryptorchidism with scrotal hyperpigmentation, labia majora containing a gonadal mass, etc. In case of any doubt, it is urgent to look for signs of a salt losing syndrome, a sign of congenital adrenal hyperplasia (see this term), the most common cause of sexual ambiguity, requiring urgent corticosteroid therapy.
If the levels of 17-OH progesterone are normal, the etiological investigation focuses on the search for drug factors during pregnancy or for a history of familial cases of ambiguity or female infertility. A series of additional examinations and medical imaging explorations are performed in order to identify the nature of the anomaly, its severity and the therapeutic strategy that can be proposed.
The etiological investigation permits to categorize the sex development disorders into three groups of unequal importance:
- 46,XX sex development disorder (60 % of cases);
- 46,XY sex development disorder (35 % of cases);
- ovotesticular disorder of sex development (5 % of cases).
In addition, chromosomal abnormalities may be the cause of sex reversal: 45X/XY mixed gonadal dysgenesis), 46XX/46XY (chimerism) and 47,XXY (Klinefelter syndrome).
|
type of ambiguity |
46,XX sex
|
46,XY sex development disorder (35 %) |
|
karyotype |
46 XX |
46 XY |
|
gonads |
2 ovaries |
2 testicles |
|
internal
|
female upto the superior third of the vagina |
variable appearance |
|
external
|
|
variable appearance |
|
cause |
hormonal hyperandrogenism |
multiple possible causes |
|
etiology |
|
|
Table: classification of the sex development disorders
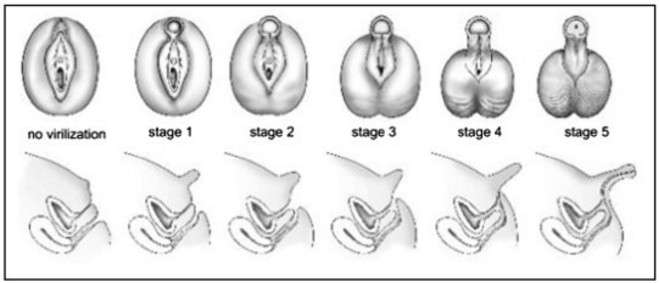
The importance of the virilization of the female genitalia is assessed by the Prader classification (table). The choice of the final sex depends on anatomical factors, the possibilities of reconstruction and the cause of the ambiguity. It is a collegial decision that must involve the parents in the final decision. The decision must be made quickly and definitively: it is absolutely necessary to avoid having to change the chosen sex.
|
Type |
Description |
|
1 |
normal vulva with clitoral hypertrophy |
|
2 |
|
|
3 |
|
|
4 |
|
|
4 bis |
absence of vaginal opening into the urogenital sinus (genitography does not opacify the vagina) |
|
5 |
|
|
5 bis |
absence of vaginal opening in the urethra. |
Prader's classification of the female sexual ambiguities
Treatment:
Surgically, it is easier to feminize (creating a vagina and reducing the size of a clitoral-penian organ) than to masculinize (it is necessary to have a penis of at least 20-25 mm in length at birth and cavernous bodies stimulated by androgens). In general, female pseudohermaphrodisms and true hermaphrodisms are surgically "feminized" and raised as girls. Male pseudohermaphrodisms pose more difficulties in the choice of the final sex and the test with androgens is a determining factor: complete or partial insensitivity to androgens, whatever the cause, imposes the female option; deficiencies in 5-alpha-reductase (see this term) are rather maintained in the male sex with dihydroandrosterone replacement therapy.
Plastic surgery of the genitalia must be performed early and, if possible, as a single procedure, based on multidisciplinary ethical considerations.
Anesthetic implications:
in case of genitoplasty: indication for a lumbar epidural block associated with general anesthesia; multiple interventions; in case of congenital adrenal hyperplasia, adapt the steroid replacement therapy (see congenital adrenal hyperplasia)
References :
- Lambert SM, Vilain EJ, Kolon TF.
A practical approach to ambiguous genitalia in the newborn period.
Urol Clin North Am 2010; 37:195-205.
- Ahmed SF, Rodie M.
Investigation and initial management of ambiguous genitalia.
Best Pract Res Clin Endocrinol Metab 2010; 24:197-218.
- Vidal I, Gorduza DB, Haraux E, Gay CL, Chatelain P, Nicolino M, Mure PY, Mouriquand P.
Surgical options in disorders of sex development (dsd) with ambiguous genitalia.
Best Pract Res Clin Endocrinol Metab 2010; 24:311-24.
Updated: December 2021