(otomandibular syndrome or dysostosis, syndrome of the first branchial arch)
See also, Goldenhar syndrome.
Prevalence: about 1/26,000 in Europe, with a slight male predominance. The cause is poorly known, but could be heterogeneous and multifactorial. The MYT1 gene (20q13.33) is thought to be responsible for a few rare cases. The lack of development of the structures of a hemiface could be secondary to a vascular problem at the level of the 1st branchial arch during embryogenesis. Hemifacial microsomia is present in many syndromes, the most common being Goldenhar syndrome, and it may be associated with a Tessier facial cleft (see this term).
The phenotypic spectrum is highly variable: from a minor isolated facial asymmetry to severe craniofacial microsomia associated with other extracranial abnormalities.
The most common manifestations are
- ear abnormalities: microtia, malposition of the ears and atresia or stenosis of the external auditory canal, with or without hearing loss
- appendages and/or pre-auricular fistulae,
- mandibular hypoplasia,
- maxillary hypoplasia,
- hypoplasia of the malar bone and/or the zygomatic arch
- ocular involvement varying from a coloboma of the upper eyelid to micro/anophthalmia
- facial paralysis, asymmetric high-arched palate, impaired extraocular movements and trigeminal nerve anesthesia have also been reported.
Other clinical signs:
- cardiac malformation: tetralogy of Fallot, VSD, ASD, transposition of great vessels, abnormalities of the aortic arch, situs inversus, dextrocardia
- renal abnormalities: unilateral renal agenesis, double ureter, renal ectopia, hydronephrosis
- central nervous system abnormalities: developmental delay, microcephaly, encephalocele, hydrocephalus, hypoplasia of the corpus callosum, Arnold-Chiari malformation, holoprosencephaly. Intelligence is usually normal.
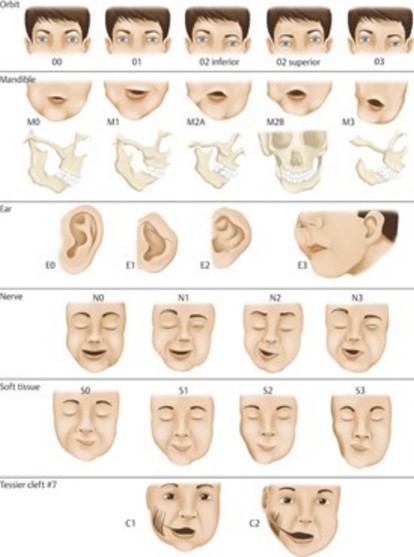
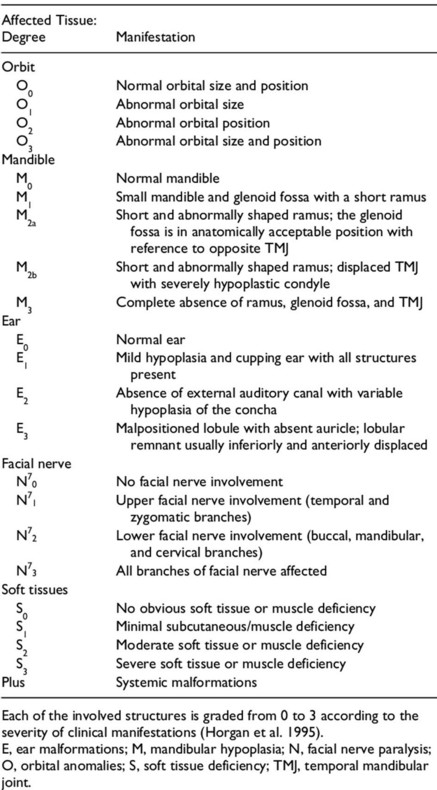
Different classifications have been proposed. The most used are OMENS+ and the Pruzanski-Hogan's one.
- OMENS+ stands for Orbit, Mandibule, Ear, Nerve (facial nerve involvement), Soft tissue and + for additional elements
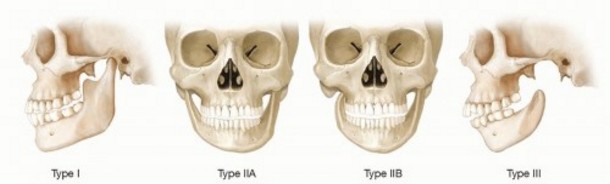
2. Pruzansky-Hogan
- I the ramus is small with an identifiable anatomy
- II the temporomandibular joint is functional but the glenoid fossa is abnormal
- IIa the glenoid fossa has an anatomically acceptable position
- IIb the glenoid fossa is in an abnormal position and cannot be incorporated into a surgical reconstruction
- III the ramus is absent and there is no glenoid fossa.
Anesthetic implications:
the presence of microtia should be a criteria to look for the presence of other signs of abnormalities of the first branchial arch: the risk of difficult mask ventilation and intubation increases with the number of items of the OMENS classification that are present: mandible ? orbit ? facial nerve ? soft tissue atrophy ? Similarly, the risk of difficult intubation increases with the importance of mandible involvement (Pruzansky-Hogan classification). The difficulty of intubation increases with age and a history of mandibular distraction does not necessarily lead to an improvement in intubation conditions.
Echocardiography. Risk of obstructive sleep apnea. Be prepared for difficult intubation: laryngeal mask, videolaryngoscope, fibroscope.
References :
- Vento AR, LaBrie RA, Mulliken JB.
The OMENS classification of hemifacial microsomia.
The Cleft Palate-Craniofacial Journal 1991: 28Ā: 68-77. - Nargozian C, Ririe DG, Bennun RD, Mulliken JB.
Hemifacial microsomiaĀ: anatomical prediction of difficult intubation.
Pediatr Anesth 1999Ā; 9Ā:393-8 - Uezono S, Holzman RS, Goto T, Nakata Y, Nagata S, Morita S.
Prediction of diificult airway in school-aged patients with microtia.
Pediatr Anesth 2001; 11:409-13 - Xu J, Deng X, Yan F.
Airway management in children with hemifacial microsomiaĀ: a retrospective study of 311 cases.
BMC Anesthesiology 2020; 20: 120, doi 10.1186/s12871-020-01038-2
Updated: December 2021