A persistent left superior vena is observed in 1.3 to 4.5% of patients with cardiopathy (versus 0.3-0.5 % in the general population), and is also more common in case of esophageal atresia. This vein, which drains the blood of left half of the head and the left upper limb, terminates in the right atrium close to the coronary sinus, which is often dilated (ultrasound). However, in about 10 % of cases, it drains into the left atrium with or without an associated fenestration of the coronary sinus (see unroofed coronary sinus): it is then a cause of desaturation by right-to-left shunting of venous blood.
This anomaly is the result of a disorder of organogenesis that occurs between the 6th and 7th week of life: normally, the cephalic end of the embryo is drained by the two anterior cardinal veins. The terminal portion of the left gets atrophied while its proximal portion drains into the right.
It is usually a fortuitous discovery when a central venous catheter is inserted by the jugular or the left subclavian route, or during cardiac catheterization. Radiologically, the central venous catheter is located to the left of the cardiac silhouette and can be advanced into the right ventricle. This last point (confirmed by a contrast opacification) allows the differential diagnosis with a intrapericardic or intrathoracic positioning or even in a collateral of the brachiocephalic venous trunk as, from left to right:
- the left mediastinal vein
- the left internal mammary vein
- the left superior intercostal vein
- the left thymic vein
If the persistence of the left superior vena cava is accompanied by an absence or hypoplasia of the right superior vena (incidence 0.1%), the pathway of the azygos vein is abnormal, which complicates the location and closure of a congenital esotracheal fistula.
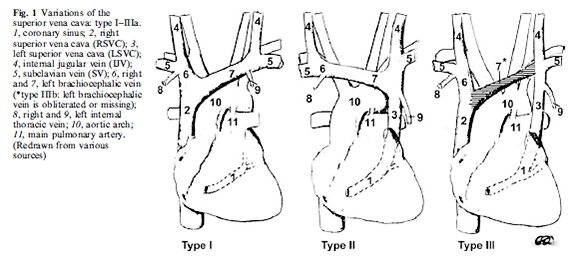
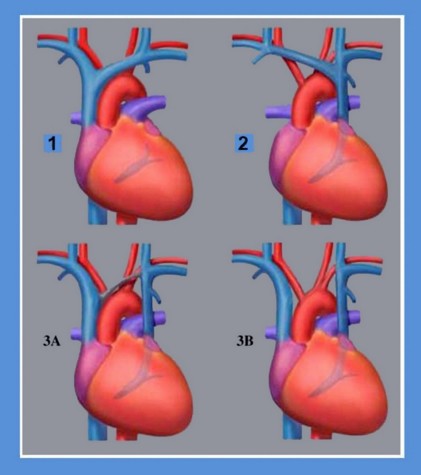
The venous drainage of superior cava can be classified as follows:
- type I: normal situation: a right superior vena cava
- type II: single left superior vena cava
- type III: presence of two superior vena cavae; IIIa if they are connected by the equivalent of an innominate venous trunk, IIIb in the absence of connection between the two veins
Anesthetic implications:
caution during the insertion of a central venous catheter from the left side in a patient with a dilated coronary sinus at echocardiography; important information to know before a cardiac bypass or creation of an cavopulmonary anastomosis (single ventricle) to ensure a good drainage of blood from the superior vena cava.
References :
- Neema PK, Manikandan S, Rathod RC.
Absent right superior vena cava and persistent left superior vena cava: the perioperative implications.
Anesth Analg 2007; 105: 40-2.
- Marret E, Meunier J-F, Dubousset AM, Pariente D, Samii K.
Diagnostic d’une veine cave supérieure gauche persistante au bloc opératoire lors d’un cathété+risme veineux central.
Ann Fr Anesth Réanim 2000 ; 19 : 191-4.
- Schummer W, Schummer C, Fröber R.
Persistent left superior vena cava and central venous catheter position: clinical impact illustrated by four cases.
Surg Radiol Anat 2003; 25: 315-21.
- Arbell D, Golender J, Khalaileh A, Gross E.
Search for the azygos : a lesson learnt from a case with left superior vena cava, esophageal atresia and tracheo-esophageal fistula.
Pediatr Surg Int 209 ; 25 : 121-2.
- Rossi UG, Rigamonti P, Torcia P, Mauri G, Brunini F, Rossi M, Gallieni M, Cariati M.
Congenital anomalies of superior vena cava and their implications in central venous catheterization.
J Vasc Access 2015Ā; 16Ā: 265-8.
- Shafiepour DS, Ladha KS, Parotto M, Paul NS, McRae KM.
Isolated persistent left-sided superior vena cava.
Anesthesiology 2017; 127: 566.
- Niyogi SG, Mandal B, Dogra N, Mishra AK.
Partial unroofed coronary sinusĀ: an uncommon cause of postcardiac surgery hypoxemia.
A&A Practice, 2020, in press
Updated: February 2020