(X0 syndrome, monosomy X, Bonnevie-Ullrich syndrome)
Prevalence: 1/2,000 to 1/3,000 female births. Gonadal dysgenesis where the caryotype is classically 45, X0 (80 %) but sometimes 46X,Xp- or 46X,Xq - (5 %) or in mosaics (15 %).
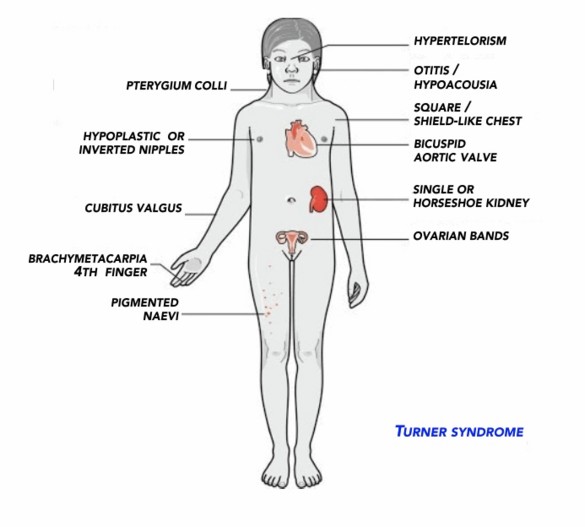
Association of:
- moderate short stature (often treatment with synthetic growth hormone), with a triangular broad chest and widely spread nipples
- dysmorphism: ptosis, low set ears, high arched palate, short neck with pterygium colli (sequelae of the cervical hygroma present in utero in the X0 forms), micrognathia,
- lymphedema of the dorsal face of the hands and feet, often present at birth and during early infancy
- cubitus valgus, scoliosis
- premature ovarian failure with absence of puberty if no substitutive treatment is started
In 40-50 % of cases, a cardiovascular anomaly is present:
- congenital heart disease: coarctation of the aorta, bicuspid aorta valve; more rarely ASD, VSD, anomalous pulmonary venous return
- progressive dilatation of the ascending aorta and dissection of the aorta especially in case of monosomy X0, which may require treatment with a β-blocker or angiotensin II receptors antagonist
- high blood pressure: very frequent, with absence of the usual nocturnal decline in BP.
One can also observe: hypothyroidism; bone deformities (scoliosis, osteoporosis); diabetes type 1 or 2 in adulthood, a 'horseshoe' kidney, an increased risk of IBD, and dermatological pathologies (numerous pigmentary nevi, psoriasis, alopecia)
Anesthetic implications:
check blood pressure; echocardiography; risk of difficult intubation, risk of bronchial intubation. Check thyroid function.
References :
- Mashour GA, Neelakantan S, Asquadro MA.
Anesthetic management of Turner syndrome : a systematic approach.
J Clin Anesth 2005; 17: 128-30.
Updated: April 2020