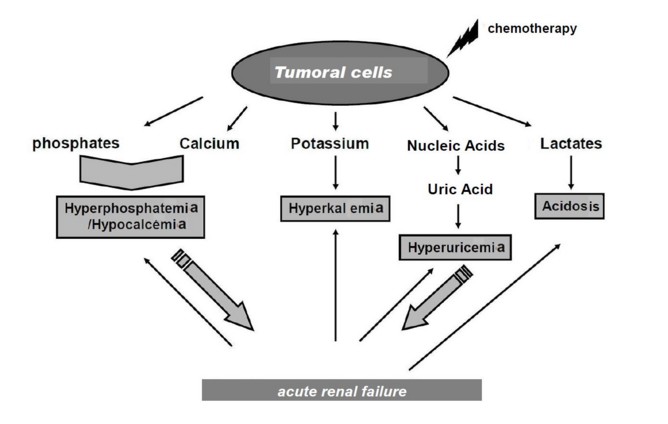
Metabolic syndrome caused by the massive release of cellular components during the lysis of malignant cells. This lysis can be spontaneous (30% of cases) or occur during the first course of chemotherapy.
Malignancies at risk are those with a fast tumor doubling rate time, e.g.: non-Hodgkin lymphoma (especially Burkitt lymphoma), all acute leukemias with major hyperleukocytosis, some solid tumors.
Two additional risk factors are:
- hyperuricemia > 450 µmol/l
- the presence of oliguria or a pre-existing renal failure due to either the precipitation of urate or phosphocalcic crystals in the renal tubules, or compression of the urinary tract (by the tumor)
The biological signs are:
- hyperuricemia > 475 µmol/L
- hyperkalemia > 6 mmol/L
- hypocalcemia < 1.75 mmol/L
- hperphosphoremia > 3mmol/L
Sometimes, an alveolar lung disease or hemostasis disorders (fibrinolysis, DIC) are associated.
Treatment:
- hyperhydration (except in case of kidney failure or oliguria): If > 10 kg: 200 ml/kg/d of a Ľ glucose 5% and ľ NaCl 0.9% mixture.
- treatment to lower hyperuricemia: urate-oxidase (rasburicase, Fastuterc®): 0.15 to 0.2 mg/kg/day IV in 30 minutes; contraindication in case of G6PD deficiency; possible side effects: respiratory distress, methemoglobinemia
- diuretics in case of insufficient diuresis
- alkalization (NaHCO3) only in case of acidosis
- normalize calcium level only if hypocalcemia is symptomatic
- extrarenal treatment (dialysis) if persistent hyperkalemia, hyperphosphoremia > 3.2 mmol/L or if [Ca x P] is < 4.6 (in mmol/L)
Anesthetic implications:
- keep this diagnosis in mind at risk situations: fast tumour growth (biopsy, installation of central catheter)
- very frequent monitoring of K, P and creatinine blood levels
- in case of cardiac arrest: to be treated as hyperkalemic until proven otherwise
- avoid any corticosteroid therapy, including the administration of low doses of dexamethasone as antiemetic, without the advice of a hematologist: cases of hyperkalemic cardiac arrest have been described.
References :
- Jabbour E, Ribrag V.
Traitement actuel du syndrome de lyse tumorale.
Revue Méd Interne 2006 ; 26 : 27-32.
- Farley-Hills E, Byrne AJ, Brennan L, Sartori P.
Tumour lysis syndrome during anaesthesia.
Pediatr Anesth 2001; 11: 233-6.
- Mc Donnel C, Barlow R, Campisi P, Grant R, Malkin D.
Fatal peri-operative tumour lysis syndrome precipitated by dexamethasone.
Anaesthesia 2008; 63: 652-5.
- Osthaus WA, Linderkamp C, Bünte C, Jüttner B, Sümpelmann R.
Tumor lysis syndrome with dexamethasone use in a child with leukemia.
Pediatr Anesth 2008; 18:268-70.
- Sinha R, Bose S, Subramaniam R.
Tumor lysis under anesthesia in a child.
Acta Anaesthesiol Scand 2009; 53: 131-3.
Updated: July 2017