(tracheal atresia)
Extremely rare malformation: estimated prevalence of 1/50,000; seems more common among males. It is generally associated with other malformations (heart, esophagus), as in VATER or VACTERL syndrome (see this term) or TACRD (acronym for Tracheal Agenesis, Radial malformation, Cardiac malformation and Duodenal atresia) :
- digestive tract (50 %): duodenal atresia, anorectal malformation
- urogenital system (35 %)
- lung (20 %): pulmonary hypoplasia
- heart (20 %): VSD, ductus arteriosus, hypoplastic left heart
- large vessels (16 %): hypoplastic aortic arch, coarctation
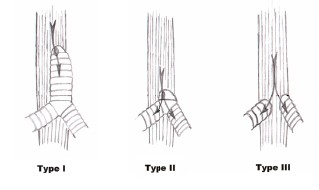
Floyd's classification is usually used to describe the anomaly: under a laryngeal or tracheal cul-de-sac, there can be
- type I (13 %): a short missing subglottic segment of the trachea; the rest of the trachea and bronchi communicates with the esophagus
- type II (65 %): the bronchi are connected to the esophagus by a short 'carina'
- type III (22 %): the bronchi opens directly into the esophagus.
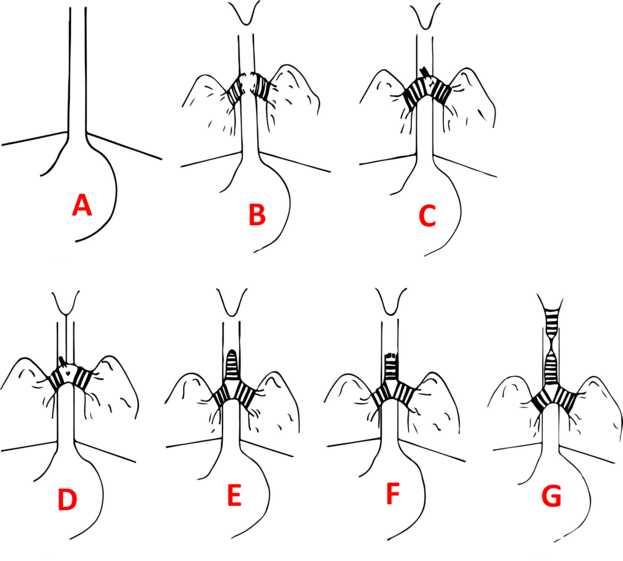
Faro's classification is more detailed but its clinical importance is relative: type A matches (lethal) with complete agenesis and the type G with a segmental congenital stenosis (see this term). Forms B (30 %), C (45 %) and E (15 %) are the most common.
The diagnosis is sometimes done in utero: presence of polyhydramnios(80 %) or CHAOS (Complete High Airway Obstruction Syndrome: hyperechogenic lungs with dil ted bronchi and flattened diaphragms) if there is no communication with the esophagus. This requires a specialized management at birth during a EXIT (EXutero Intrapartum Therapy) procedure.
Clinically, the malformation results in acute respiratory obstruction after the clamping of the umbilical cord. The newborn makes considerable inspiratory efforts but is unable to inhale air or scream. If the lesion is a suspected or known, the baby should be ventilated by mask and intubated via the esophagus or use a supraglottic device. Mortality at 1 year of age: 92,6 %.
Anesthetic implications:
birth by EXIT in case of antenatal diagnosis
It is important to quickly make the differential diagnosis between tracheal agenesis and atresia of the larynx as their immediate support (at birth) is different:
- laryngeal atresia : cyanosis with fruitless inspiratory efforts; mask ventilation and intubation are difficult or impossible; mask ventilation is possible only in case of associated esophageal-tracheal fistula associated; treatment: emergency tracheotomy.
- tracheal agenesis : immediate respiratory distress and absence of cry but ventilation by mask is possible; impossible intubation of a apparently normal larynx; treatment: intubate the esophagus and leave the newborn breathing spontaneously to prevent abdominal distension: this enables survival if the esotracheal or esobronchial communication is sufficiently large; later, intubation of the trachea by rigid esophagoscopy (type I and II) or feeding gastrostomy and ligation of the lower esophagus (type III). Otherwise tracheotomy at birth.
Complex reconstructive surgery of the trachea.
References :
- Haben M, Rappaport JM, Clarke KD.
Tracheal agenesis.
J Am Coll Surg 2002 ; 194 : 217-22.
- Manschot HJ, Van Den Anker JN, Tibboel D.
Tracheal agenesis.
Anaesthesia 1994; 49: 788-90.
- Soh H, Kawahawa H, Imura K, Yagi M et al.
Tracheal agenesis in a child who survived 6 years.
J Pediatr Surg 1999; 34: 1541-3.
- van Veenendaal MB, Liem KD, Marres HA.
Congenital absence of the trachea.
Eur J Pediatr 2000; 159:8-13.
- Shimabukuro F, Sakumoto K, Masamoto H, Asato Y, Yoshida T, Shinhama A, Okubo E, Ishisoko A, Aoki Y.
A case of congenital high airway obstruction syndrome managed by ex utero intrapartum treatment: case report and review of the literature.
Am J Perinatol. 2007; 24:197-201.
- Kohl T, Van de Vondel P, Stressig R, Wartenberg HC, Heep A, Keiner S, Müller A, Franz A, Fröhlich S, Willinek W, Gembruch U.
Percutaneous fetoscopic laser decompression of congenital high airway obstruction syndrome (CHAOS) from laryngeal atresia via a single trocar--current technical constraints and potential solutions for future interventions.
Fetal Diagn Ther 2009; 25:67-71.
- Saleeby MG, Vustar M, Algren J.
Tracheal agenesis: a rare disease with unique airway considerations.
Anesth Analg 2003; 97:50-2.
- Baroncini-Cornea S, Gargiulo G, Gentili A, Lima M et al.
Tracheal agenesis : management of the first 10 months of life.
Pediatr Anesth 2004; 14: 774-7.
- Heimann K, Bartz C, Naami A, Peschgens T, Merz U, Hörnchen H.
Three new cases of congenital agenesis of the trachea.
Eur J Pediatr 2007; 166:79-82.
- Dijckman KP, Andriessen P, van Lijnschoten G, Halbertsma FJ.
Failed resuscitation of a newborn due to congenital tracheal agenesis: a case report.
Cases Journal 2009; 2: 7212.
- Bober K, Musialik-Swietlinska E, Adamiec-Poniewierka E, Pajak J, Bjelecki I et al.
Tracheal agenesis: perioperative management of one stage correction.
Pediatr Anesth 2008; 18: 982-3.
- Sattler C, Chiao F, Stein D, Murphy D.
Life-saving esophageal intubation in neonate with undiagnosed tracheal agenesis: a case report.
A&A Case reports 2017; 9: 31-4.
- Smith MM, Huang A, Labbé M, Lubov J, Nguyen LHP.
Clinical presentation and airway management of tracheal atresia: a systematic review.
Int J Pediatr Otorhinolaryngol 2017; 101:57-64.
- Willer BL, Bryan KG, Parakininkas DE, Uhing MR, Staudt Sr et al.
Anesthetic management of an infant with postnatally diagnosed tracheal agenesis undergoing tracheal reconstruction : a case report.
A&A Case reports 2017; 9: 311-8.
- Gonzalesa SK, Goudyb S, Prickettb K, Ellis J.
EXIT (ex utero intrapartum treatment) in a growth restricted fetus with tracheal atresia.
Int J Pediatr Otorhinolaryngol 2018 ; 105 : 72-4.
Updated: July 2024