Rare malformation usually due to presence of complete O-shaped tracheal rings. Sometimes isolated, often associated with other malformations either cardiac (especially of the aortic arch) or in the context of a VATER or VACTERL syndrome (see this term).
There are 3 types of congenital stenosis of trachea (Cantrell's and Guild's classification):
a) generalized hypoplasia: 30 %
b) funnel stenosis: 20 %
c) segmental stenosis: 50 %, generally due to the presence of a few complete tracheal rings. This type has been later subdivided as type 3 (presence of a tracheal bronchus and involvement of the carina), type 4 (no tracheal bronchus and normal carina), type 5 (localised to the carina) and type 6 (presence of a single lung) (Anton Pacheco)
.jpg)
.jpg)
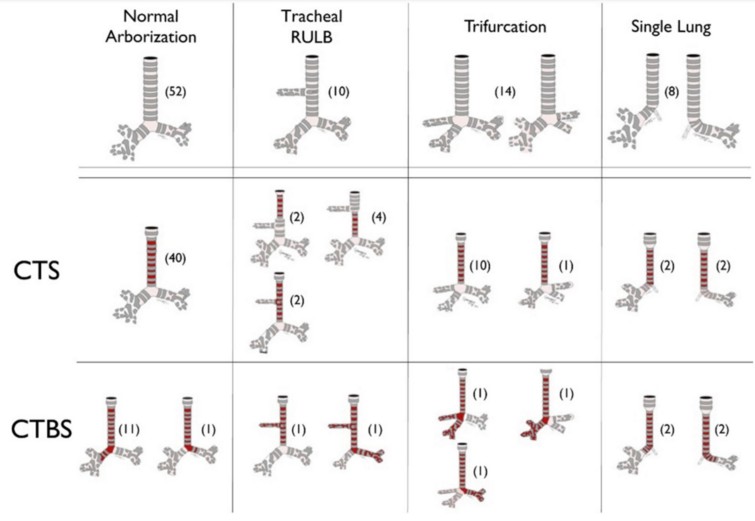
A 3rd classification, the Great Ormond classification, has been proposed in 2012: it considers the type of division of the trachea (normal, tracheal bronchus, tracheal trifurcation, agenesis of the main bronchus) and the possible association with a bronchial stenosis.
Symptoms: depending on the importance of the stenosis, respiratory distress at birth, respiratory failure during an upper airway infection, inspiratory and expiratory stridor, incidental finding during intubation.
Treatment: resection-anastomosis in case of segmental involvement; some teams try endoscopic dilatations of the trachea, but those are poorly successful in the presence of complete tracheal rings. Slide-tracheoplasty for the more extended forms.
Anesthetic implications:
- keep this pathology in mind in case of difficult intubation despite an easy laryngoscopy in a newborn or infant with a cardiopathy, or suffering of a VATER/VACTERL syndrome; keep a supraglottic airway ready and different very small diameter tubes to bypass the stenosis; emergency ORL examination to establish a diagnosis ( congenital or acquired stenosis, extrinsic compression, significant tracheomalacia)
- in case of intubation where the endotracheal tube is maintained above the stenosis (segmental form), it is prudent to leave a distance of about 1 cm between the distal end of the tube and the beginning of the stenosis to avoid edema or other local traumatic lesions
- for repair: cardiopulmonary bypass, ECMO, or high frequency ventilation; in some cases, wait for the tracheal incision before injecting the myorelaxant and controlling ventilation
- for peripheral surgery: keep a supraglottic airway ready, associated if possible with locoregional anesthesia ; keep at hand different very small diameter tubes to bypass the stenosis (e.g., suction or ureteral catheter)
- if the child has been operated for a tracheal stenosis: use, if possible, a supraglottic airway; atraumatic intubation !
References :
- Murphy PM, Lloyd-Thomas A.
The anaesthetic management of congenital tracheal stenosis.
Anaesthesia 1991; 46: 106-9.
- Takasaki Y, Hayashi Y, Takadi O, Uchida O, Kuro M.
Unexpected congenital tracheal stenosis in infants with congenital heart disease.
Anesth Analg 1993; 77: 198-9.
- Concha M, Gonzalez J, Gonzalez A, Dagnino R, Molina R.
Epidural anaesthesia for ureteral reimplantation in an infant with congenital tracheal stenosis.
Can J Anaesth 1997; 44: 666-8
- Li Y, Khambatta HJ, Stone JG, Mets B.
Unsuspected concentric tracheal rings in a 14-year-old with scoliosis.
British J Anaesth 2002; 88 : 732-4
- Ali MI, Brunson CD, Mayhew JF.
Failed intubation secondary to complete tracheal rings: a case report and literature review.
Pediatr Anesth 2005; 15: 890-2
- Taylor K, Levine M.
Management of congenital tracheal stenosis: using spontaneous ventilation to facilitate cardiopulmonary bypass.
Pediatr Anessth 2006; 16: 492-5.
- Sacco O, Toma P, Alberti D, Locatelli G et al.
Inspiratory stridor in a 12 month-old girl.
Pediatrics Intern 2007; 49: 10122-4
- Speggiorin S, Torre M, Roebuck DJ, McClaren CA, Elliott MJ.
A new morphologic classification of congenital tracheobronchial stenosis.
Annals Thor Surg 2012; 93: 958-61
- De Cloedt L, Papadopoulos J, Corouge P, Khalil P, Van Laer P.
Hypoplasie trachéale complexe chez un enfant de 2 mois.
Arch Pédiatr 2013 ; 20 : 1321-4.
- Obara S, O’Leary JD.
Congenital tracheal stenosis : unanticipated and anticipated difficult airway management in a neonate.
Anesth Analg Case Reports 2014; 3: 120-2
- Mauron S, Longchamp D, Perez M-H, Prętre R, Sandu K, De Bernardo S, Boegli Y, Dolci M.
Anesthetic management for concomitant correction of congenital cardiac defects and long “O” ring tracheal stenosis: a role for heliox? Report of 2 cases.
A&A Practice 2018; 10: 154-6
- Yokoi A, Hasegawa T, Oshima Y, Higashide S et al.
Clinical outcomes after tracheoplasty in patients with congenital tracheal stenosis in 1997-2014.
J Pediatr Surg 2018; 53: 2140-4.
Updated: July 2023