Prevalence of 1 in 3000 births. They are as common as duodenal atresia. The most commonly cited pathophysiologic mechanism is acute vascular insufficiency during pregnancy resulting in segmental intestinal necrosis. There exist a very rare form, called familial multiple intestinal atresia [MIM 243 150], due to autosomal recessive transmission of a mutation of the TTC7A gene (2p16), associated with moderate immunodeficiency.
Unlike duodenal atresia, small bowel atresia and stenosis is rarely associated with other malformations.
The main associated anomalies are:
- polyhydramnios: 25 % of cases
- prematurity: 50 % of cases
- intrauterine volvulus: 27 % of cases
- cystic fibrosis: 11.7 % of cases
- laparoschisis: 16 % of cases.
Clinical forms:
- stenoses: localized narrowing of the intestinal lumen without any loss of continuity and with an intact mesentery. The stenosed segment usually consists in has a thickening and irregularities of the muscularis mucosae. The cause of stenosis is can sometimes a digestive duplication.
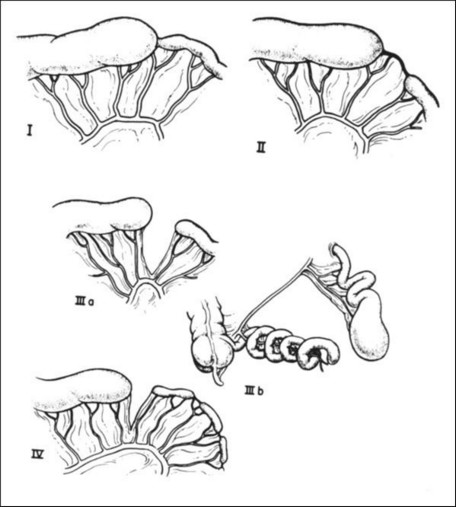
- atresias are more severe malformations that can be categorized into 4 types:
- type I: localized diaphragm-shaped thickening of the mucosa and sub-mucosa that causes a localized obstruction with upstream intestinal dilation and downstream microilia; the mesentery is intact and the length of the small bowel is normal;
- type II: the intestinal continuity is interrupted and the proximal, extremity is dilated and connected, via a fibrous cord, to a the downstream segment of reduced diameter; the mesentery is intact and the total length of the small bowel is usually normal;
- type III: the overall appearance is similar to type II, but there is no fibrous cord connecting the two separate intestinal segments; there is a "V"-shaped dehiscence of the mesentery and the total length of the intestine is shortened; this type is often divided into 2 subtypes, depending on the extent of intestinal shortening and abnormalities of the mesenteryĀ:
- IIIa: simple interruption of the mesentery, with an almost normal length of the small bowel
- IIIb: often described as "Christmas tree" or "apple peel" because the distal intestine wraps around a single mesenteric vessel and forms a spiral while the proximal segment is only vascularized by a small right ileocolic or colic artery due to partial agenesis of the superior mesenteric artery; there is often an associated colonic malrotationĀ; prognosis is severe in terms of morbidity (risk of short bowel syndrome) and mortality, especially since it is often associated with prematurity;
- type IV: the intestinal continuity is interrupted in several places and may involve each of the three previous types of atresia; the anatomical aspect is that of a "sausage rosary"; the cause is unknown, but the hypothesis of multiple intrauterine ischemic episodes at an early stage of the digestive tract development is favoured.
The prenatal diagnosis is possible in only 30-40 % of cases, mainly in extensive forms of atresia. The symptomatology at birth depends on the severity of the malformation. It may be limited to episodes of intermittent vomiting and lack of satisfactory weight gain or present bilious vomiting with abdominal distension within hours of birth.
Plain abdominal X-ray shows liquid levels but it is the contrast enema that allows the best diagnostic orientation by showing a microcolon and the eliminating other diagnoses (such as Hirschprung's disease).
The prognosis depends on the length of the residual small bowel (risk of short-bowel syndrome) and the quality of the mesenteric vascularisation. It is usually very good in type I to IIIa forms but the morbidity (28 % for short-term and 17 % for long-term complications) and the mortality (11 %) are high, mainly in type IIIb and IV forms.
Anesthetic implications:
- preoperative: gastric tube to decompress the abdomen, hydroelectrolytic and metabolic resuscitation, broad-spectrum antibiotic prophylaxis, and search for possible associated malformations
- neonatal anesthesia: modified rapid sequence induction, risk of hypotension, hypothermia, hypoxemia (ductus arteriosus and foramen ovale still patent)
- postoperative gastric drainage as the resumption of intestinal transit is often slow and straining of the digestive sutures should be avoided.
- in the absence of sepsis at the time of surgery, epidural analgesia is a good option.
ReferencesĀ:
- Stollman TH, de Blaauw I, Wijnen MH, van der Staak FH, Rieu PN, Draaisma JM, Wijnen RM.
Decreased mortality but increased morbidity in neonates with jejunoileal atresia; a study of 114 cases over a 34-year period.
J Pediatr Surg 2009; 44:217-21.
Updated: January 2020