It is the most common congenital malformation of the pancreas. It occurs in 4 to 14 % of subjects. It results from an anomaly in the fusion of the dorsal and ventral pancreatic ducts, which occurs early in the embryogenesis of the pancreas. Along with other anatomical variations of the pancreatic excretory ducts, this anomaly belongs to the dominant dorsal pancreatic duct syndrome, in which the dorsal duct is said to be dominant because it drains most of the pancreatic parenchyma through a non-adapted accessory papilla.
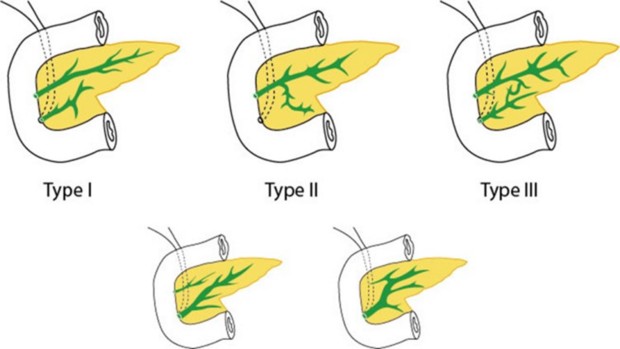
There are 3 types in which the dorsal pancreatic duct drains dominantly or exclusively through the accessory papilla:
- Type I: complete pancreas divisum (71 %): the dorsal duct drains most of the pancreas and terminates in the accessory papilla; the ventral duct drains part of the pancreatic head and terminates in the main papilla.
- Type II: isolated dorsal duct (23 %): the ventral duct does not drain into the duodenum. It may even be completely absent.
- Type III: incomplete pancreas divisum (6 %) or predominant Santorini duct: fusion between the two ducts is incomplete or rudimentary, and takes place via a fine secondary duct, which is not very functional.
Other embryological anomalies of pancreatic duct fusion have no clinical expression:
- inverted pancreas divisum: the accessory pancreatic duct does not connect with the genu of the main pancreatic duct.
- isolated ventral duct: in this form, the accessory pancreatic duct does not terminate in the duodenum.
Clinical presentation: most patients are asymptomatic; 5 % of cases present with acute pancreatitis: it is undoubtedly the association with stenosis of the accessory papilla that is at the root of the pathogenic effects. This disease should be investigated in cases of recurrent idiopathic acute pancreatitis. Pancreas divisum may also be complicated by chronic abdominal pain or chronic obstructive pancreatitis.
Diagnosis: retrograde cholangiography, cholangiowirsungo-MRI.
Treatment: in cases of idiopathic acute recurrent pancreatitis, endoscopic sphincterotomy of the minor papilla or surgical sphincteroplasty may be considered.
Anesthetic implications:
none outside episodes of pancreatitis.
References :
- Neblett WW, O’Neill JA Jr.
Surgical management of recurrent pancreatitis in children with pancreas divisum.
Ann Surg. 2000;231 :899-908.
Updated: December 2023