(congenital microvillous atrophy, Davidson disease, DIAR2)
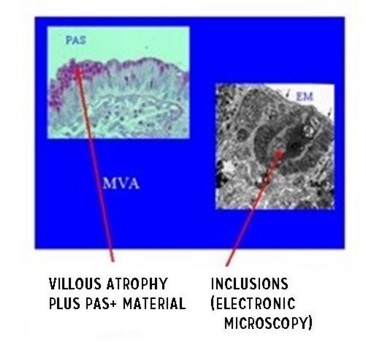
Prevalence: < 1/106. Probably autosomal recessive transmission of a mutation of gene MYO5B (myosin Vb) (18q21.1) which plays an important role in cell polarity. Some cases could be due to a mutation of the RAB8-GTPase . Congenital anomaly of the intestinal epithelium resulting in watery diarrhea (up to 250 to 300 ml/kg/d of stool) which compromises the vital prognosis. It begins either in the first days of life (early form), or within the first two months (late-onset form). Some forms are pseudoobstructive and difficult to differentiate from chronic intestinal pseudoobstruction (see this term). Classical microscopy shows accumulation of PAS-positive granules at the level of the apical pole of immature enterocytes, and atrophy of the microvilli of the mature enterocytes with one PAS- or CD10-positive intra-cellular line that corresponds to microvillous inclusions at electronic microscopy.
Ultrastructural analyses reveal:
1) partial or total atrophy of the microvilli of the mature enterocytes and apical accumulation of secretory granules in immature enterocytes
2) characteristic inclusion bodies containing rudimentary or well differentiated microvilli in mature enterocytes.
The intestinal failure secondary to diarrhea is definitive. There is no cure and the children are completely dependent on parenteral nutrition. The long-term prognosis is bad due to the metabolic and renal problems (nephrocalcinosis), repeated episodes of dehydration, and infectious and hepatic complications (either due to an familial intrahepatic cholestasis with normal serum level of γGT, or secondary to parenteral nutrition). Early intestinal transplantation is a factor of hope in the treatment and prognosis of this disease.
Anesthetic implications:
check hydration, electrolytes and liver function. Risk of post-infectious thrombosis of central venous catheters (echoguided placement)
References :
- Goldman LJ, Lopez Santamaria M, Gamez M.
Anaesthetic management of a patient with microvillus inclusion disease for intestinal transplantation.
Pediatr Anesth 2002; 12: 278-83
- Ruemmele FM, Schmitz J, Goulet O.
Microvillous inclusion disease (microvillous atrophy).
Orphanet J Rare Dis. 2006;1:22.
- Sayar E, Kalay S, Yilmaz A et al.
Microvillus inclusion disease associated with necrotizing enterocolitis in a premature infant.
Am J Perinatology Reports 2014; 4: e61-3
Updated: October 2016