Term used to describe an anomaly of closure of the spinal canal that could have led to the formation of a meningocele, if its evolution had not been interrupted by intradural fixation of the nervous structures by dorsal adhesions. These adhesions are fibrous bands or abnormal nerve roots that bind the medulla, the nerve roots or the filum terminale and the inner surface of the dural sac. Depending on their location, these adhesions cause a posterior shift of the medulla, the cauda equina and or the filum terminale that is visible at MRI. These anomalies are more frequent at the lumbar level, but have been described at all levels of the neuraxis.
In 30 to 40 % of cases, these intradural adhesions go through the dura and extend to the extradural space, the vertebral laminae or even subcutaneously.
There may be ventral intradural adhesions in case of type 2 diastematomyelia (= without separation of the two spinal cords by a bony spur) (see this term).
Signs and symptoms depend on the location and importance of the adhesions. In the absence of skin changes (40 % of cases), the diagnosis is often late (around 11 years of age) on the basis of the appearance of abnormal reflexes in one or both limbs, urinary incontinence, spasticity.
Cutaneous anomalies: tuft of hair, hemangioma, dermal sinus, 'cigarette paper-like' scar on the skin overlying the neuraxis, subcutaneous lipoma, dermoid cyst.
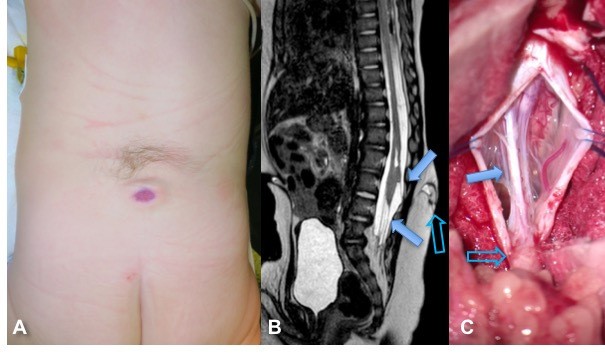
Meningocele manqué with dystrophic skin and hyperpilosity (A); (B) MRI shows the skin lesion (open arrow) in continuity with the intra-dural band (upward arrow); the filum terminale is also tense; C: operating view showing the point of dural penetration of the band (hollow arrow) and its intradural pathway with adhesions to the spinal cord (arrow) (Source: Professor M. Vinchon, neurochirurgiepediatriquelille.com)
Anesthetic implications:
all skin anomalies located on the spinal axis should be considered as suspicious, and raise the possible diagnosis of spinal anomalies such as a tethered spinal cord. Regional echography during the neonatal period often allows the diagnosis of a concealed anomaly. MRI is necessary for accurate diagnosis. Contraindication to a neuraxial block.
References :
- Aquilina A, Galea G, Grech R.
Meningocele manqué.
BMJ Case Rep 2017; doi: 10.1136/bcr-2017-220213
- Schmidt C, Bryant E, Iwanaga J, Oskouian RJ et al.
Meningocele manqué: a comprehensive review of this enigmatic finding in occult spinal dysraphism.
Childs Nerv Syst 2017; 33: 1065-71.
Updated: February 2019