[MIM 241 500, 241 510, 146 300]
(Rathburn disease, phosphoethanolaminuria)
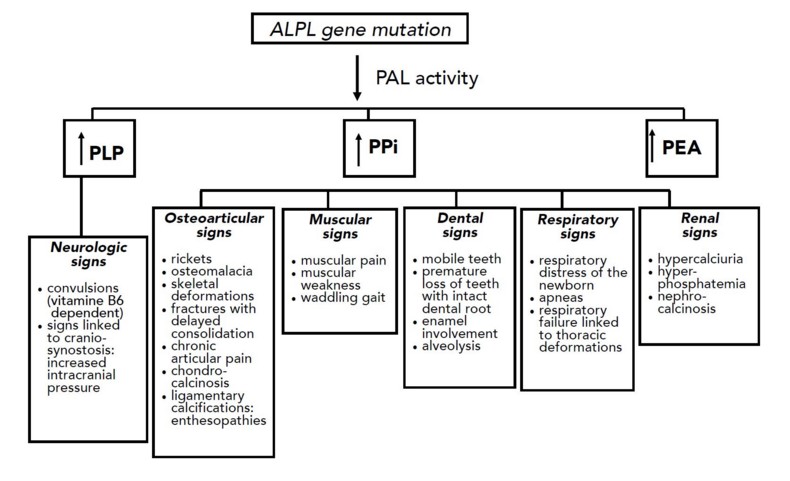
Very rare: estimated prevalence of 1/100,000 for the severe forms and 1/6,000 for the mild forms and 1/2,500 in Mennonite families in Manitoba. Autosomal recessive, sometimes dominant transmission of a mutation of the ALPL gene (1p36.1-34) that causes hypomineralisation of bones and teeth as a result of the deficiency ofa non-specific alkaline phosphatase especially expressed in the liver, kidney, bone, neurons, and neutrophils. There is an increase in osteoid tissue that contains a large amount of non-mineralized extracellular matrix (without hydroxyapatite crystals) that produces osteomalacia and rickets. This non-specific alkaline phosphatase is involved in the synthesis of GABA as it is necessary for the dephosphorylation of pyridoxal-5'-phosphate, derived from vitamin B6: this GABA deficiency explains epileptic seizures in some patients. The clinical presentation is very variable depending on the mutation and the resulting residual enzyme activity.
Réf.: adapted from Debiais F. in Revue du Rhumatisme Monographies 2019; 86:31-9.
Based on the clinical presentation, there are:
- a lethal perinatal form: short and deformed limbs, membranous cranium, not mineralized ribs, resulting in rapid respiratory failure; epileptic seizures
- a mild perinatal form: similar signs on prenatal ultrasound as the lethal form but with a better prognosis
- an infantile form (first signs before the age of 6 months): signs of rickets, , distorted limbs and ribs, sometimes craniosynostosis (40 %), hypercalciuria with nephrocalcinosis: the main risk is respiratory failure
- a juvenile form (first signs between 6 months and 18 months of age): deformed limbs (at the level of the extremities of the long bones), delayed walking, waddling walking, craniosynostosis, rapid muscle fatigue, premature loss of the deciduous teeth
- an adult form (after 18 years of age): premature fall of deciduous teeth in clinical history, very painful osteomalacia with stress fractures (metatarsals), osteoarthropathies
- a dental form or odontohypophosphatasia with only premature fall of teeth and caries
.jpg)
Juvenile form
Treatment: daily supplements of vitamin B6 and enzyme substitution with asfotase alpha by subcutaneous injection (6 mg/kg once a week or 2 mg/kg 3 times a week)
Anesthetic implications:
bone pain responding well to NSAIDS; fragile bones (! positioning); fragile teeth; in case of craniosynostosis, risk of intracranial hypertension
References :
- Orimo H.
Pathophysiology of hypophosphatasia and the potential role of asfotase alfa.
Therapeutics and Clinical risk management 2016; 12:777-86.
- Nahabet EH, Gatherwright J, Vockley J, Henderson N, Tomei KL et al.
Postnatal pancraniosynostosis in a patient with infantile hypophosphatasia.
Cleft Palate Craniofacial J 2016; 53: 741-4
- Rougier H, Desrumaux A, Bouchon N, Wroblewski I et al.
Enzyme-replacement therapy in perinatal hypophosphatasia: case report and review of literature.
Arch Pédiatr 2018; 325: 442-7
Updated: November 2021