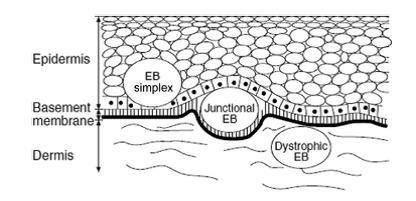
Prevalence: 1/1x106 live births. Fragility of the skin that form bubbles when subjected to a force of friction or shear, or minor trauma. More than 20 forms have been described. A group of international experts has classified them into 4 types according to the layer of the skin where the erosion or the bubble appears: basal layer (simple epidermolysis), clear layer (stratum lucidum) (junctional epidermolysis), dense layer (dystrophic epidermolysis), or several levels (Kindler syndrome). It is very difficult to make an accurate diagnosis (electron microscopy, immunofluorescence, mutations) in the neonatal period.
There are specifically:
- simple bullous (EB Simplex) or epidermolytic (or intraepidermal) epidermolyses: onset at birth or during the neonatal period except the localized form that appears in childhood. PHP1 and DSP genes are involved in the suprabasal forms and KRT5, KRT14, PLEC1, ITGA6 and ITGB4 genes in basal forms.
|
layer |
NAME |
autosomal transmission |
OLD name |
bulles |
extracutaneous signs |
|
|
lethal acantholytic |
recessive |
|
|
- |
|
supra
|
deficiency in phakolin |
recessive |
|
none : superficial erosions |
- |
|
|
superficial EBS |
recessive |
|
|
- |
|
|
localized EBS |
dominant |
Cockayne-Weber |
++++
|
- |
|
|
Dowling-Meara (DM) |
dominant |
|
++++ herpetiform aspect of the bullae |
- occasional oropharyngeal lesions |
|
|
generalized non-DM |
dominant |
Koebner |
++++ |
- |
|
basal |
with pigmentation |
dominant |
|
++++ |
- |
|
|
with muscular dystrophy |
recessive |
|
++++ |
- late dystrophy |
|
|
with pyloric atresia |
recessive |
|
++++ |
- |
|
|
autosomal récessive |
recessive |
|
+++ |
- anemia, growth retardation |
|
|
Ogna |
dominant |
|
+++ |
- |
|
|
migratory circinate |
dominant |
|
++++ |
- |
- junctional epidermolysis (Lamina lucidolytic EB) : autosomal recessive transmission. Onset at the neonatal period, except for the late form which starts in adulthood; the genes involved are LAMA3, LAMB3, LAMC2, COL17A1, ITGB4 and ITGA4.
Here are the different types:
|
types |
NAME |
bullae |
extracutaneous lesions |
vital pronostic |
|
Herlitz |
lethal atrophic epidermolysis of Herlitz |
++++ |
anemia nail abnormalities growth retardation enamel hypoplasia digestive & respiratory & ocular and urogenital lesions, pseudosyndactylies |
bad |
|
|
atrophic epidermolysis known as benign (non-Herlitz) or generalized |
++++ |
anemia nail abnormalities growth retardation enamel hypoplasia digestive & respiratory & ocular and urogenital lesions |
reserved |
|
|
localized |
++ |
enamel hypoplasia |
good |
|
Non-Herlitz |
with pyloric atresia |
++++ |
enamel hypoplasia |
bad |
|
|
inverse |
+++ in the folds |
enamel hypoplasia |
good |
|
|
late onset |
++ |
enamel hypoplasia |
good |
|
|
LOC syndrome (Shabbir) |
++ with érosions |
face, larynx, teeth |
bad |
- dystrophic or dermatolytic (Dermolytic EB) epidermolysis: the most serious forms of EB. autosomal dominant or recessive transmission of a mutation in the COL7A1 gene; onset: neonatal or during infancy blisters heal leaving atrophic scars and contractures; oral, pharyngeal and esophageal (stenosis) lesions, pseudosyndactyly, corneal erosions. Chronic pain related to the blisters and treatments (cfr burned patients). Malnutrition and esophageal stenoses often necessitate the use of a gastrostomy (ideally by laparoscopic approach).
|
transmission |
NAME |
OLD name |
bullae |
extracutaneous lesions |
vital pronostic |
|
|
generalized |
Pasini Cockayne-Touraine |
+++ |
digestive lesion |
|
|
|
pretibial |
|
++++ tibias, feet, hands |
- |
good |
|
|
pruriginous |
|
++++ |
- |
good |
|
dominant |
limited to the nails |
|
none, nails dystrophy |
- |
good |
|
|
limited to the extremities |
|
++++ feet, hands |
- |
good |
|
|
neonatal bullous dermolysis |
|
+++ |
- |
good |
|
|
generalized severe |
Hallopeau-Siemens |
++++ |
digestive and ocular lesions, pseudosyndactylies |
bad + spinocellular |
|
|
generalized |
non-Hallopeau-Siemens |
++++ |
|
reserved + spinocellular |
|
recessive |
inverse |
|
+++ folds, paravertebral |
anemia growth retardation urogenital and digestive lesions |
|
|
|
pretibial |
|
++++ tibias, feet, hand |
- |
good |
|
|
limited to the extremities |
|
++++ feet, hands |
- |
good |
|
|
pruriginous |
|
++++ |
- |
good |
|
|
centripetal |
|
+++ tibias, feet, hands |
- |
|
|
|
neonatal bullous dermolysis |
|
+++ |
- |
good |
- Kindler syndrome (Mixed EB): rarest form; autosomal recessive transmission of a mutation of the KIND1 or FERMT1 gene (20p12. 3) coding for kindline-1, a protein that links the actin cytoskeleton to the extracellular matrix; neonatal onset; bullae all over the whole body surface; progressive improvement with age, but secondary keratoderma and discrete interdigital webbing; photosensitivity; few or no extracutaneous lesions: colitis, esophagitis; early and severe periodontitis, pitted amelogenesis imperfecta of variable severity, gingival hyperplasia; sometimes cicatricial microstomia; vital prognosis is relatively good.
Increased risk of skin carcinoma (basal cell carcinoma).
Anesthetic implications:
echocardiography to detect any dilated cardiomyopathy (by dietary deficiency in selenium and/or carinitine, chronic anemia, iron overload); the dystrophic forms as well as the simple ones due to a mutation of the KHLH24 gene are at increased risk.
Risk of difficult intubation; microstomia, trismus, ankyloglossia. Frequent dental decay. Risk of laryngeal lesions anywhere alongside the glottis. Risk of esophageal stenosis.
For all forms, there is extremely fragile skin and mucous membranes (except the nasal mucosa): avoid any friction or shear as this causes the formation of blisters. Desinfection by dabbing. No adhesive, no ECG electrodes except if the skin is protected by Mepiform® Mepilex® or Mepitel®. The interposition of a hydrophilic gel plate (such as those used to ensure a good skin conduction during defibrillation: 3M® Defib pads 2346N) between the ECG electrodes or diathermy plate has been used with success. Difficult venous access. No diathermy plate (prefer bipolar coagulation). In general, there is a chronic use of ointments containing cortisone: risk of adrenal insufficiency, osteoporosis. If possible: IV induction; if inhalatory induction, oral premedication to avoid any hyperexcitation; cover the face mask with petrolatum or KY soaked compresses; careful lubrication of laryngoscope blades, gloves, laryngeal mask etc. in case of blisters: pierce them with a sterile needle. Avoid skin infiltration with local anesthetic (for dental care e.g.) as the mechanical effect is similar to a shear but regional blocks (axillary, epidural, spinal anesthesia) have been used with success. Use non-adhesive dressings type Aquacel® Mepiform® or Mepitel®. Avoid plaster, suppositories, lollipops. A silicone spray TrioNiltac® can be used to remove the dressings.
For junctional forms: respiratory impairment (25% of cases) is generally linked to severe forms and associated with gastroesophageal reflux. The Herlitz type presents the highest risk for complications: the risk of laryngeal stenosis is ± 40 % at the age of 6 years. It presents as weak and hoarse voice, stridor, respiratory distress. It can however be treated endoscopically but it is not uncommon to have to perform a tracheostomy.
For dystrophic forms: difficult intubation (opening of the mouth limited by retractile scars); it seems preferable to use the nasal route to intubate (wuth a well lubricated tube softened in hot water) because the endonasal epithelium is of respiratory origin and more resistant to shear forces.
An experimental treatment based on Beremagene Geperpavec gel (Vyjuvek®) (max 0.6ml/week if < 6 months, max 1.6 ml/week if > 6 months). This is a gene therapy using herpes virus type 1 as a vector for the normal COL7A1 gene, with promising results in forms linked to a COL7A1 gene mutation.
The affected skin surface and the metabolic needs required by healing can result in a loss of fluids, hypoproteinemia and malnutrition, with pharmacological consequences.
The intranasal route has been used successfully to obtain rapid analgesia.
The importance of the pain and itching is very variable. Pruritus is often resistant: try anti- histaminics, tricyclic antidepressants, pregabalin, ondansetron, methylnaltrexone, lidocaine gel.
In case of epidermolysis bullosa simplex, daily use, for 15-20 minutes long dressingg changes, of an equimolar mixture of oxygen and nitrous oxide has proved effective for several months and without producing adverse effects if vitamin B12 supplementation and regular monitoring of blood levels of folic acid and vitamin B12 is provided.
Website: www.debra-international.org.uk
References :
- Fine JD, Eady RA, Bauer EA, Bauer JW, Bruckner-Tuderman L, Heagerty A, Hintner H, Hovnanian A, Jonkman MF, Leigh I, McGrath JA, Mellerio JE, Murrell DF, Shimizu H, Uitto J, Vahlquist A, Woodley D, Zambruno G.
The classification of inherited epidermolysis bullosa (EB): Report of the Third International Consensus Meeting on Diagnosis and Classification of EB.
J Am Acad Dermatol 2008; 58:931-50. - Herod J, Denyer J, Goldmann A, Howard R.
Epidermolysis bullosa in children; pathophysiology, anaesthesia and pain management.
Pediatr Anesth 2002; 12: 388-97. - Lin Y-C, Golianu B.
Anesthesia and pain management for pediatric patients with dystrophic epidermolysis bullosa.
J Clin Anesth 2006; 18: 268-71. - Edler AA, Ramamurthi RJ, Valenzuela GA.
Improving electrical safety for patients with Epidermolysis bullosa.
Pediatr Anesth 2008; 18: 1107-9 - Englbrecht JS, Langer M, Hahnenkamp K, Ellger B.
Axillary plexus block in a child with dystrophic epidermolysis bullosa.
Anaesth Intensive Care 2010; 38: 1101-5.
- Chang T.
Skin fragility and blister formation.
JAMA 2011; 306: 767-8.
- Ida JB, Livshitz I, Azizkhan RG, Lucky AW, Elluru RG.
Upper airway complications of junctional epidermolysis bullosa.
J Pediatr 2012; 160: 657-61. - Aronson LA.
Images in Anesthesiology : Child with junctional epidermolysis bullosa, hoarseness, and nasal obstruction demonstrating laryngeal stenosis.
Anesthesiology 2016 ; 125 :1044. - Ingelmo P, Wei A, Rivera G.
Nitrous oxide for procedural analgesia at home in a child with epidermolysis bullosa.
Pediatr Anesth 2017 ; 27 : 776-8 - Araujo M, Bras R, Frada R, Guedes-Martins L, Lemos P.
Caesarean delivery in a pregnant woman with epidermolysis bullosa: anaesthetic challenges.
Int J Obst Anaesth 2017; 30: 68-72. - Strupp KM, Zieg JA, Johnson B, Szolnoki JM.
Anesthetic management of a patient with epidermolysis bullosa requiring major orthopedic surgery: a case report.
A&A Practice 2017; 9: 73-6. - Bowen L, Burtonwood MT.
Anaesthetic management of children with epidermolysis bullosa.
BJA Education 2018; 18: 41-5 - Stoopler M, Vigouroux M, Mohamed N, Macabuag Y, Ingelmo P.
Long-term efficacy and adverse effects of outpatient procedural analgesia with nitrous oxide for a child with Epidermolysis Bullosa.
Pediatr Anesth 2022; 32:85–7. - Mittal BM, Goodnough CL, Bushell E, Turkman-Bazzi S, Shepparrd K.
Anesthetic management of adults with epidermolysis bullosa.
Anesth Analg 2022; 134:90-9 - Brooks Peterson M, Strupp KM, Brockel MA, Wilder MS, Zieg J, Bruckner AL, Kaizer AM, Szolnoki JM.
Anesthetic management and outcomes of patients with epidermolysis bullosa: experience at a tertiary referral center.
Anesth Analg 2022; 134:810-21. - Mughal AZ, Subramanian T, Jones R, James D, Ogboli M, Soccorso G.
Evaluating the use of laparoscopic-assisted gastrostomy tube feeding in children with epidermolysis bullosa: A single-center retrospective study.
J Pediatr Surg 2022 ; 57 : 39-44 - Guide SV, Gonzalez ME, Bgci IS, Agostini B, Chen H, Feeney G, Steimer G et l.
Trial of Beremagene Geperpavec (B-VEC) for Dystrophic Epidermolysis Bullosa.
N Engl J Med 2022; 387:2211-9 - Krämer S, Hillebrecht AL,Wang Y, Badea M-A, Barrios JI, Danescu S, Fuentes I, Kartal D, Klausegger A, Ponce de León E, Schilke R, Yordanova I, Bloch-Zupan A, Has C.
Orofacial anomalies in Kindler Epidermolysis Bullosa.
JAMA Dermatol. doi:10.1001/jamadermatol.2024.0065
Updated: May 2025