(MIM 126800, 604356)
(DRS, Duane retraction syndrome)
Congenital form of strabismus characterized by a limitation of horizontal eye movements: attempting to adduct the eye cause narrowing of the palpebral fissure and retraction of the eyeball in the orbital cavity. It is responsible for about 1 % of the strabismus and is classified as strabismus abducens with possible fibrosis of extraocular muscles (while the anomaly is neurological). The majority of cases are sporadic but cases with autosomal dominant transmission (2-3%) have been reported. Many loci (encoding for the brainstem nuclei which are absent or hypoplastic) have been associated with this syndrome. Several genes (DURS1 on 8q13, DURS2 on 2q31, SALL4 on 20q13) have been identified. This syndrome may be due to an abnormality of the innervation coming from the brainstem so that the lateral rectus muscle of eye is partially innervated by branches of the common oculomotor nerve. Abnormalities of the vertical movement of the eye may be associated. The diagnosis is usually made around the age of 10 years.
There are 3 types:
- type I (70-90 %): it is mainly the abduction which is compromised
- type II: adduction is not possible
- type III (15 %): adduction and abduction are very limited.
Each type is in turn divided into 3 subgroups depending on the gaze direction when the patient looks ahead: A the affected eye is deviated towards the nose (esotropia), B, the affected eye is diverted in direction of the ear (exotropia) and C, no deviation.
The involvement is bilateral in 10 to 20 % of cases. It can be associated with other ocular abnormalities (coloboma, Marcus Gunn, amblyopia, dysplasia of the iris, Morning Glory) (30 %) or other syndromes (Goldenhar, Holt-Oram, Klippel-Feil, Dandy-Walker, Okihiro, conduction deafness).
This anomaly requires surgical correction in case of compensatory torticollis or amblyopia.
Anesthetic implications:
ensure that this syndrome is not part of another syndrome (Goldenhar, Dandy-Walker, Holt-Oram, Okihiro, Klippel-Feil syndrome); if this is the case, this syndrome-specific anesthetic considerations are prevailing since the isolated form of Duane syndrome does not imply specific anesthetic considerations outside the fact to be more careful about the clinical assessment of the depth of anesthesia (position of the eyeballs can not be relied on).
References :
- Alexandraxis G, Saunders RA.
Duane Retraction syndrome.
Ophtalmol Clin North America 2001; 14: 407-17.
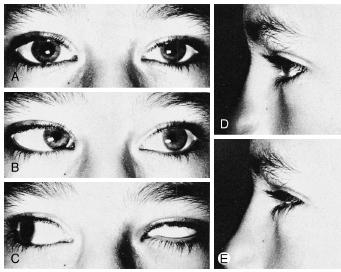
Duane I syndrome of the left eye
Updated: August 2019