Warning: do not mix up with double outlet right ventricle !
A congenital heart disease in which the aorta and pulmonary artery originate totally or in part from the right ventricle and produce a mixed shunt.
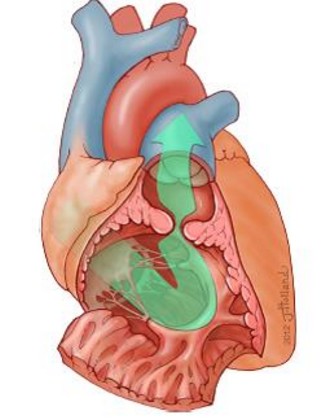
Incidence: between 0.5 and 2 % of all cardiac malformations. Often diagnosed during adolescence but adult cases are also described. Cardiac malformation characterized by the division of the right ventricle in two chambers by anomalous muscle bands in the right ventricular outflow tract: a proximal high-pressure one, close to the tricuspid valve, and a distal, low-pressure one, close to the pulmonary valve (picture). An infrafundibular intraventricular pressure gradient greater than 20 mmHg is considered as abnormal). It is associated with other cardiac malformations (mainly a VSD, tetralogy of Fallot, Ebstein’s anomaly) in 80-90 % of cases. Some experts think that it could be an acquired malformation: the turbulent flow created in the right ventricular outflow tract in the presence of a VSD could trigger abnormal hypertrophy of part of the interventricular septum (septal marginal trabecula, crista supraventricularis, moderator band).
Its clinical presentation is highly variable and depends on the importance of the intraventricular obstruction: exertional dyspnea, chest pain, syncope.
Clinical examination: ejection systolic murmur in the left parasternal area.
EKG: right ventricular hypertrophy
Diagnosis: transthoracic echocardiograph is poorly contributive due to limited visualization of the right ventricle: transoesophagel echocardigraphy, MRI or cardiac catheterization are often necessary.
Treatment: depending on the symptoms; β-blockers, surgical resection of the abnormal musculofibrous bands (when pressure gradient is > 40 mmHg or in case of heart failure).
Anesthetic implications:
recent cardiac echography, maintain β-bloquing or calcium channel blockers up to the day of anesthesia, avoid using inotropes (that could increase the dynamic component of the intraventricular obstruction), optimal right ventricular preload. After corrective surgery, a right bundle branch block or ventricular arrhythmias may occur.
References:
- Loukas M, Housman B, Blaak C, Kralovic S et al.
Double-chambered right ventricle: a review.
Cardiovascular Pathology 2013; 22: 417-23
- Moustafa S, Patton DJ, Alvarez N, Al Shanawani M et al.
Double chambered right ventricle with ventricular septal defect in adults: case series and review of literature.
J Cardiovasc Ultrasound 2015; 23: 48-51
- McNeil JS, Vergales JE, Bechtel AJ, Kleiman AM.
Double-chambered right ventricle.
Anesthesiology 2019; 130: 150-1
UpdateĀ: March 2019