(laryngeal cleft)
Rare. Congenital anomaly due a lack of separation of airway and digestive tract at the level of the larynx and sometimes the trachea induced by the cranial growth of tracheo-esophageal septum: the earlier the stop, the more severe is the defect.
The classification of Benjamin and Inglis is used:
- occult type: only submucosal laryngeal diastema , asymptomatic;
- type I: inter-arytenoid defect
- type II: defect which extends to the level of the cricoid,.
- type III: defect extending along the entire cervical trachea (6th tracheal ring);
- type IV: defect that extends into the thoracic trachea (sometimes up to the carena or a bronchus).
- type IVb: defect that extends into the bronchus
This malformation is often associated with:
- a Opitz-Frias syndrome (or G syndrome)
- Pallister-Hall syndrome
- CHARGE syndrome
- esophageal atresia in 6 % of cases, isolated or in a VATER association.
Clinically: symptoms difficult to distinguish from an esophageal-tracheal fistula with or without atresia of esophagus, gastroesophageal reflux, a paralysis of the vocal cords or a swallowing incoordination: stridor, a hoarseness, an hypersialorrhea, shortness of breath, trouble swallowing with cough and cyanosis, especially during feeding trials, repeated pulmonary infections.
In moderate forms (types I and II), the diagnosis is based on a careful laryngoscopy showing a posterior inter-arytenoid slot that may go unnoticed if one does not use a palpateur or a tracheoscope to explore the posterior laryngeal commissure. In severe forms, the initial diagnosis is often made when an endotracheal tube positioned between the vocal cords can be found in the esophagus.
The definitive treatment is to separate the trachea of the esophagus and several approaches are possible depending on the type of diastema:
- pharyngo-oesophagoplasty by the cervical route,
- pharyngo-laryngo-oesophagoplasty by anterior sternotomy, thoracotomy or thoracoscopy or by a combined cervical and thoracic approach
- endoscopic surgery (laryngoscopy in suspension) in case of type I resistant to medical treatment, type II and type III: in these cases, a TIVA based propofol or dexmedetomidine and remifentanil titrated so as to preserve the CPAP is the technique recommended by the team of Boston: a constant supply of O2 is provided via a probe attached to the tip of the laryngoscope and which can serve as a probe of insufflation for a jet-ventilation in case of temporary apnea
Anesthetic implications:
- - initial attitude: protect the airway to secure the ventilation and avoid pulmonary regurgitations. The easiest way is to insert a urinary catheter into the stomach and inflate the balloon; a slight but constant traction is applied on the proximal end of the catheter to occlude the cardia, which allows to ventilate the child by intubation or laryngeal mask, and to wait for the baby to grow. Alimentation is supplied via the gastrostomy) until an extensive evaluation of the problem is made.
- - reconstructive surgery: surgery reserved for highly trained teams. Depending on the extent of lesions, control of the airway during reconstructive surgery can be assured by a tracheostomy, unipulmonaire ventilation or by a double lumen "tailor-made" tube. Outside the types I and II, morbidity and postoperative mortality (infection, fistula) are important.
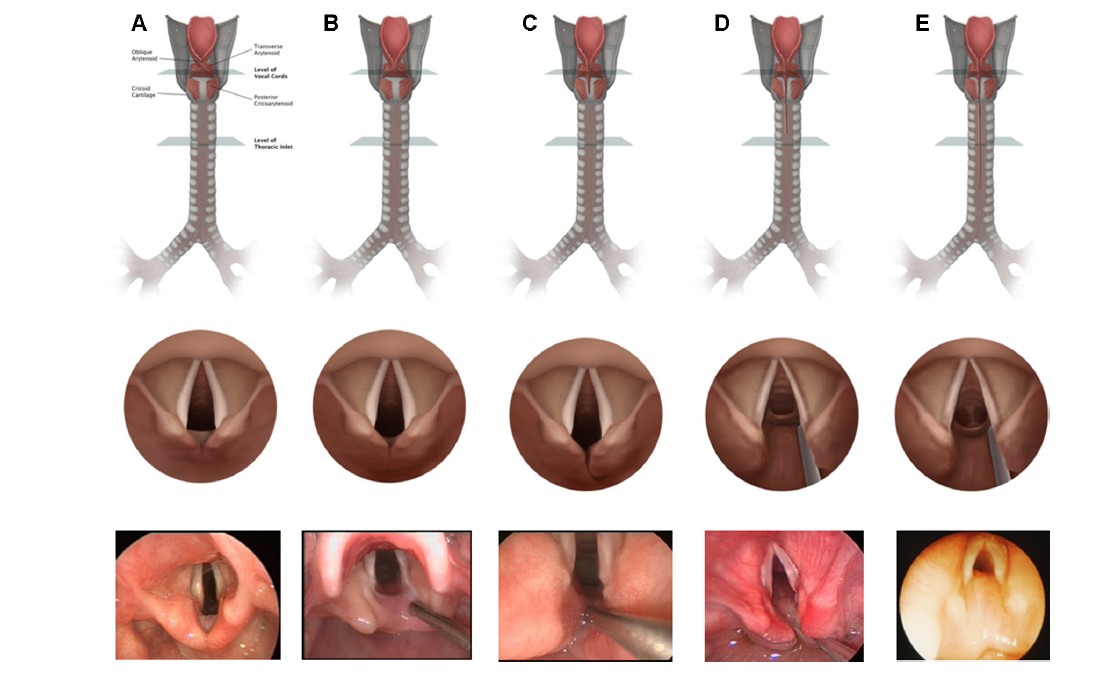
A: normal: B: type I, C: type II, D: type III, E: type IV
References :
- Carr MM, Clarke KD, Webber E, Giacomantonio M.
Congenital laryngotracheoesophageal cleft.
J Otolaryngol 1999; 28:112-7. - Arai LR, Dicindio S, Cook SP, Davis DA.
Anesthesia management of a patient with a laryngotracheo-esophageal cleft.
Pediatr Anesth 2007; 17: 171-5. - Jöhr M, Berger TM, Ruppen W, Schlegel C.
Congenital laryngotracheo-oesophageal cleft: successful ventilation with the laryngeal mask airway.
Paediatr Anaesth 2003; 13:68-71. - Russell P, Chambers N, du Plessis J, Vijayasekeran S.
Emergency use of a size 1 laryngeal mask airway in a ventilated neonate with an undiagnosed type IV laryngotracheo-oesophageal cleft.
Paediatr Anaesth. 2008; 18:658-62. - Tagawa T, Ukoda M, Sakuraba S.
Anesthetic management of a neonate with type IV laryngotracheo-esophazgeal cleft.
Pediatr Anesth 2009; 19:792-4. - Fernandez A, Jerez A, Falcone N.
Anaesthetic management in a case of a type IV laryngotracheo-oesophageal cleft.
Paediatr Anaesth 2003; 13:270-3. - Ahmad R, Sami KA, Rabeeah A.
A bifurcated endobrochial tube in the management of laryngotracheo-oesophageal cleft repair.
Br J Anaesth 1993; 70:696-8. - Vas L, Patil B, Ragavendra S, Hosalkar H, Pratibha G.
Complications of anaesthesia and surgery for laryngotracheo-oesophageal cleft.
Paediatr Anaesth 2001; 11:361-5. - Ferrari L, Zurakowski D, Solari J, Rahbar R.
Laryngeal cleft repair : the anesthetic perspective.
Pediatr Anesth 2013 ; 23 : 334-41 - Johnston DR, Watters K, Ferrari LR, Rahbar R.
Laryngeal cleft: evaluation and management.
Int J Pediatr Otorhinolar 2014; 78: 905-11. - Vuncannon J, Albanna M, Evans AK.
The adaptive use of a hand-crafted endotracheal-endobronchial tube for airway management in laryngo-tracheo-oesophageal cleft type IV.
Int J Pediatr Otorhinolaryngol 2017; 98: 71-4.
Updated: November 2017