(Middle aortic syndrome)
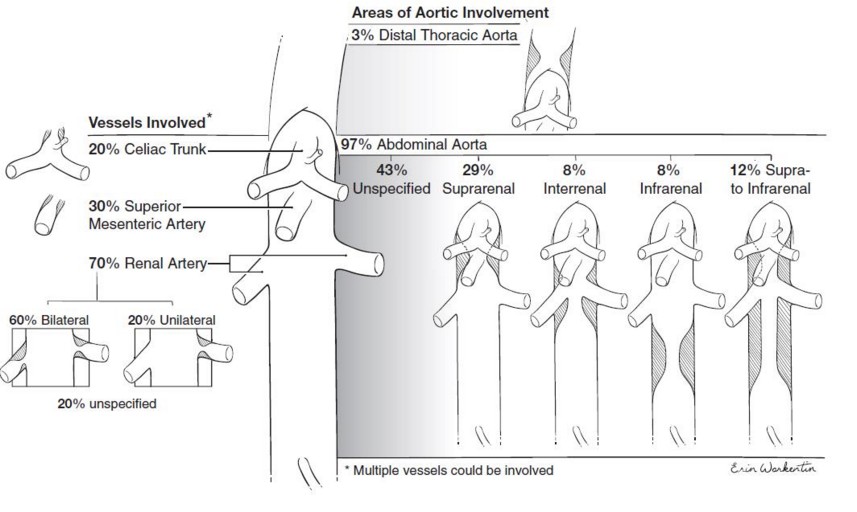
Rare: represents 0.5 to 2 % of the coarctations of the aorta. Severe, segmental or diffuse stenosis, of the descending aorta at the thoracic and/or abdominal level. Often associated with involvement of other arteries: renal (70 %), upper mesenteric or celiac. The table reports the distribution in 630 published pediatric cases.
The cause is:
- idiopathic (63 %): the site is most often infrarenal; could be due to an abnormality of the fusion of the embryonic dorsal primitive aortae.
- genetic (15 %): as in Alagille, Turner or Williams-Beuren syndrome, neurofibromatosis type I, Moyamoya disease (see these terms); the site is most often suprarenal; the renal and mesenteric vessels are involved in 60-70 % of cases. There is a carotid or retinal involvement in 10 % of cases.
- inflammatory (17 %): arteritis such as in Takayasu disease. The abdominal involvement is generally isolated in that case.
- fibrodysplasia
Presentation: high blood pressure of renovascular origin in the majority of cases, weak or absent femoral pulses, presence of an abdominal murmur, post-prandial abdominal pain (mesenteric angina), intermittent claudication
Evolution: LVH, early atheromatosis, sometimes cardiac failure or stroke
Treatments: antihypertensive drugs, endoluminal dilation with or without stenting, surgical treatment (bypass), renal auto-transplantation
Anesthetic implications:
hypertension (ECG, echocardiography, fundoscopy), renal function, blood typing and crossmatching in case of vascular surgery (risk of hemorrhage, rupture); central venous actheter and direct monitoring of the arterial blood pressure; in case of surgery: management of aortic clamping/unclamping. CSF drainage to protect the spinal cord perfusion (as in case of thoracic aortic aneurysm in adult) does not seem to be useful.
References :
- Connolly JE, Wilson SE, Lawrence PL, Fujitani RM.
Middle aortic syndrome: distal thoracic and abdominal aortic coarctation, a disorder with multiple etiologies.
J Am Coll Surg 2002; 194: 774-81
- West CA, Delis KT, Service GJ, Driscoll DJ, McPhail IR, Gloviczki P.
Middle aortic syndrome: surgical treatment in a child with neurofibromatosis.
J Vasc Surg 2005; 42: 1236.
- Rumman RK, Nickel C, Matsuda-Abedini M, Lorenzo AJ, Langlois V et al.
Disease beyond the arch: a systematic review of Middle Aortic Syndrome in children.
Am J Hypertension 2015; 28: 833-46
- Forman N, Sinskey J, Shalabi A.
A review of middle aortic syndromes in pediatric patients.
J Cardiothorac Vasc Anesth 2020;34: 1042-50.
- Rajakaruna R, Porter KR, Ok MS.
Mid-aortic syndrome.
Anesthesiology 2021; in press
Updated: April 2021