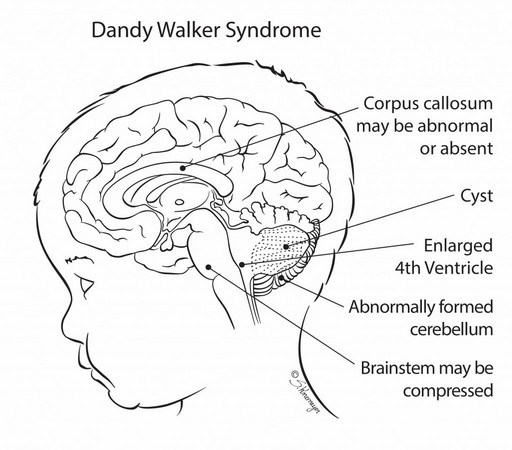
Incidence 1/100,000 live births, more common in boys (1.24 per 100,000) than girls (0.78 per 100,000). This malformation is the cause of 3.5% of infantile hydrocephalies. It is by definition the association of hydrocephaly with partial or complete agenesis of the cerebellar vermis and a cyst in the posterior fossa in communication with the fourth ventricle. In case of normal communication between the fourth ventricle and the arachnoid spaces and simple hypoplasia of the vermis, it is identified as a Dandy Walker variant but this is presently controversial. The etiology is heterogeneous:
- recessive autosomal transmission when it is part of some polymalformative syndromes (Meckel or Joubert) or in case of some metabolic diseases (CDG syndrome),
- autosomal dominant transmission: G syndrome
- X-linked transmission: Aicardi syndrome
- sporadic association with a chromosomal aberration.
- of teratogenic origin: maternal diabetes, maternal viral disease, drugs.
Clinical presentation:
- early onset hydrocephalus with bulging occiput, rapid increase in head circumference, then appearance of symptoms of obstructive hydrocephalus (4%)
- signs of involvement of the posterior fossa
- in general: delayed motor development, and cerebellar dysfunction with loss of balance and coordination, nystagmus, cranial nerve paralysis.
- sometimes completely asymptomatic.
Another congenital anomaly is associated, in about 30 % of cases:
- facial dysmorphism: micrognathia, cleft palate, macroglossia, hypertelorism
- syndactyly
- cardiopathy
- agenesis of the corpus callosum
Sometimes associated facial anomalies: micrognathia, cleft palate, hypertelorism. Sometimes: syndactyly, congenital heart disease, agenesis of the corpus callosum.
X-Ray: footprints at the level of the transverse sinuses with reduction in thickness and curvature of the occipital bone.

Anesthetic implications:
risk of intracranial hypertension; in 50 % of cases, abnormalities of brainstem function: apnea, vocal cords paralysis and swallowing disorders, increased risk of laryngospasm (?); risk of difficult intubation; micrognathia; occipital limiting deformity the extension of the neck
References :
- Ewart MC, Oh TE.
The Dandy-Walker syndrome. Relevance to anaesthesia and intensive care.
Anaesthesia 1990; 45:646-8.
- Khan A, Kurtz B, Ambardekar A.
Lessons learned from a burn-injured pediatric patient with Dandy-Walker syndrome after multiple anesthetics: a case report.
A&A Practice 2019;13:166-8.
Updated: June 2021