(pericardial agenesis, CAP)
Very rare: unknown prevalence (0,007 to 0,015 % of autopsies) because the defect is often asymptomatic. Total or partial absence (usually on the left side) of the pericardium is due to a failure of separation between the pericardial and pleural cavities around the 7th week of intrauterine life. When the fusion defect is small, it is identified as a pleuropericardial fistula. When one side of the pericardium is absent, this results in homolateral pleurocardial cavity. In order of frequency, the left pericardium is most often absent (70 %). The right pericardium is involved in 17 % of cases and the involvement is bilateral in 9 % of cases.
The absence of pericardium is associated with another malformation in 30 to 50 % of cases:
- cardiac malformation: ASD, ductus arteriosus, tetralogy of Fallot, abnormal pulmonary venous return, mitral pathology
- in case of association of the absence of the pericardium with and a left diaphragmatic hernia, there is a significant risk of subluxation of the heart in the left hemithorax, or even outside the thorax after the repair of the diaphragmatic defect. In case of association with a defect in the thoracoabdominal wall, it is a variant of Cantrell's pentalogy (see this term).
- bronchogenic cyst, bronchial sequestration, VACTERL or Pallister-Killian syndrome (see these terms)
- marfanoid collagen diseases
- sometimes observed in cases of type A aortic dissection: no tamponade but massive left hemothorax.
The normal pericardium is an avascular fibrous sac consisting of an internal serous layer and an external fibrous layer attached to the diaphragm and the sternum. The serous layer consists of a visceral membrane attached to the epicardium and a parietal part attached to the fibrous sac; they are separated by a few ml of serous fluid. The fibrous sac stabilizes the position of the heart in the chest and the serous membranes have a lubricating role to avoid friction on the cardiac surface during the heartbeats.
- bilateral or total left pericardial agenesis: it is generally better tolerated than partial agenesis. It is often asymptomatic or causes chest pains that can mimic other heart conditions (atypical angor, tumor). The apical impulse is displaced to the left. ECG: electric alternance, slow progression of the R wave. Echography: difficult because the usual axis of vision are maladjusted to the position of the cavities and their unusual mobility. Chest X-Ray and MRI: left position of the cardiac silhouette; presence of pulmonary tissue (air) between the aortic arch and the trunk of the pulmonary artery (A).
- Partial agenesis: atypical chest pains that are often positional and paroxysmal, not related to stress, sometimes sudden death. Medium-sized defects have a risk of herniation of an auricle (B) or all or part of an atrium, or part of a ventricle (cardiac strangulation), causing a situation of compression of the coronary arteries. A typical sign is trepopnea, i.e. the presence of dyspnea when the patient is lying on one side (left in case of left partial defect) and not on the other side. Symptomatic patients require treatment: closure or enlargement of the defect, pericardectomy or pericardoplasty.
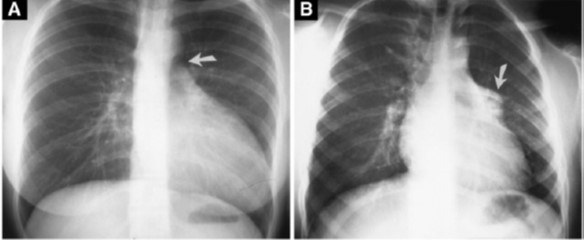
A: total absence of pericardium: interposition of pulmonary tissue between the aorta and the pulmonary artery
B: partial absence of the left pericardium: hernia of the left auricle in the thoracic cavity
Anesthetic implications:
generally none except in case of subluxation of the heart in the thoracic cavity; sometimes poor tolerance of the left lateral decubitus
ReferencesĀ:
- Verloes A, Perrin L, Delbecque K, Gonzales M, Demarche M, Dekoster G.
Congenital absence of the left pericardium and diaphragmatic defect in sibs.
Eur J Med Genet 2010; 53:133-5.
- Lopez D, Asher CR.
Congenital absence of the pericardium.
Progress in Cardiovasc Dis 2017; 398-406.
- Shah AB, Kronzon I.
Congenital defects of the pericardium.
Eur Heart J 2015; 16:821-7.
- Nicholas J, Barber E, Grondin S, Haber J.
Congenital absence of the pericardium encountered during thoracoscopy.
Can J Anesth 2022Ā: 69Ā:898-9.
Updated: July 2022