Acronym for Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy.
Prevalence estimated at 4/100,000, but variants associated with CADASIL but without clinical manifestations are found in around 2 to 10/1000 individuals. It is a specific non-atheromatous arteriopathy (granular deposits in the arteriolar wall), leading to subcortical infarcts and white matter lesions. It is caused by the autosomal dominnat transmission of variants of the NOTCH3 gene (19p.13.2-p13.1), whose locus is close to that of the CACNL1A4 calcium channel, mutations of which cause familial hemiplegic migraine. It generally manifests itself from the third decade onwards as atypical migraines, auras without headaches, or migraines with hemiplegia, epilepsy and early dementia. There is often a history of migraines in childhood.
The pathology appears to be due to cerebral hypoperfusion, mainly affecting subcortical regions and white matter. The cerebrovascular response to changes in paCO2 is thought to be diminished, but cerebral autoregulation appears to be preserved, at least in the early stages of the disease.
Diagnosis: genetics, skin biopsy.
A severity score based on the MRI image has recently been established for this disease and other arteriopathies linked to a mutation in the NOTCH3 gene:
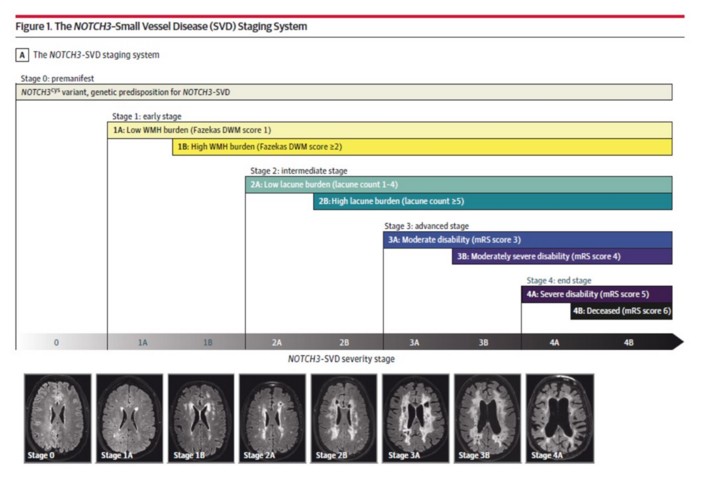
The radiological elements included in this severity score are the Fazekas score for deep white matter hyperintensity, the number of lacunae and the modified Rankin scale (mRS), which measures the severity of disability following a stroke.
Progressive worsening of dementia. Increased risk of sudden cardiac death, partly associated with reduced heart rate variability, a sign of cardiac autonomic dysfunction.
Treatment: antiaggregant dose of aspirin; antiepileptics in case of epilepsy; sometimes acetazolamide (carbonic anhydrase inhibitor).
Anesthetic implications:
dementia, epilepsy; maintain cerebral perfusion pressure within the normal limits for the patient: avoid hypo- and hypercapnia, as well as hypo- and hypertension. It may be useful to use NIRS to assess cerebral (cortical!) oxygenation and rapidly detect hypoperfusion in the monitored zone (measure values in the vigorous state). Monitoring the depth of anesthesia (BIS, for example) is of little use in avoiding peranesthetic arousal, but it is undoubtedly useful to know the BIS on awakening in the event of dementia.
References :
- Cleves C, Friedman NR, Rothner AD, Hussain MS.
Genetically confirmed CADASIl in a pediatric patient.
Pediatrics 2010; 126: e 1603-7.
- Dieu JH, Veyckemans F.
Perioperative management of a CADASIL type arteriopathy patient.
Br J Anaesth 2003 ; 91: 442-4.
- Pfefferkorn T, von Struckrad-Barre S, Herzog J, Gasser T, Hamann GF, Dichgans M.
Reduced cerebrovascular CO2 reactivity in CADASIL: a transcranial Doppler sonography study.
Stroke 2001; 32: 17-21.
- Singhal S, Markus HS.
Cerebral reactivity and dynamic autoregulation in nondemented patients with CADASIL (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy).
J Neurol 2005; 252: 163-7.
- Rufa A, Guideri F, Acampa M, Cevenini G et al.
Cardiac autonomic nervous system and risk of arrhythmias in Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL).
Stroke 2007; 38: 276-80.
- Lamberg JJ, Cherian VT.
Neuraxial anesthesia in CADASIL syndrome.
J Neurosurg Anesthesiol 2013; 25: 216.
- Rasooli S, Moslemi F, Tagavi S.
Anesthetic management and postoperative care of a patient with CADASIL (Cerebral Arteriopathy, Autosomal Dominant, with Subcortical Infarcts and leukoencephalopathy) for cesarean section.
International Journal of Women’s Health and Reproduction Sciences 2014 ; 2 : 326–8
- Bermúdez-Triano M, Guerrero-Domínguez R, Martínez-Saniger A, Jiménez I.
General anesthesia considerations in CADASIL disease.
Revista Espańola de Anestesiología y Reanimación (Engl Edi), 2019 ; 66 : 226-9
- Gravesteijn G, Rutten JW, Cerfontaine MN, Hack RJ, Liao Y-C, Jolly AA, Guey S et al.
Disease severity staging system for NOTCH3-associated small vessel disease, including CADASIL.
JAMA Neurol. 2025;82: 49-60. doi:10.1001/jamaneurol.2024.4487
Updated: January 2025