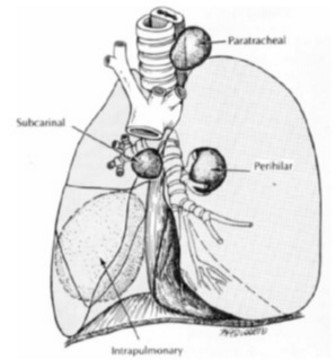
The most common form of congenital lung cysts. It represents 6 to 15 % of mediastinal masses in children. It is the consequence of the development of an autonomic bud from the primary pulmonary tissue, before the formation of the tracheobronchial tree: it can be intrapulmonary (27 %), mediastinal (65 %) (it is then called neuroenteric cyst) or in the triangular ligament (7 %). The usual localization is in the median mediastinum, near the carina. Cervical localization is rare and often confused with a thyroglossal cyst.
Intrapulmonary cysts often communicate with the bronchial tree and are lined with a respiratory epithelium and filled with mucus. They are often asymptomatic.
Chest X-ray or CT scan: rounded opacity of variable size, full or airy with a liquid level if there is communication with the bronchial tree.
Neuroenteric cysts present in the same appearance as bronchogenic cysts but in the posterior mediastinum and communicate with the spinal canal which is frequently abnormal.
Surgical indications (thoracotomy or thoracoscopy) are made in the presence of clinical symptoms such as respiratory distress, infection, purulent sputum, hemoptysis or pneumothorax. Some cysts have a malignant potential, especially in the form of pleuropulmonary blastoma (see this term), which should lead to early surgery before 2 years of age.
Differential diagnosis: adenomatoid malformation of the lung, pulmonary sequestration, pneumatocele, pulmonary echinococcosis
Anesthetic implications:
echocardiography: compression of large vessels ?
Induction of anesthesia should be made in the best tolerated position by the patient (sometimes the supine position is poorly tolerated because cough or dyspnea); risk of contamination of the healthy lungs in case of communication with the bronchial tree.
Hemorrhagic risk. Decide with the surgeon whether one lung ventilation is required.
References :
- Birmingham PK, Uejima T, Luck SR.
Anesthetic management of the patient with a bronchogenic cyst: a review of 24 cases.
Anesth Analg 1993;76:879–83.
- Politis GD, Baumann R, Hubbard AM.
Spillage of cystic pulmonary masses into the airway during anesthesia.
Anesthesiology.1997; 87:693–6.
- Kiran M, Thotungal R, Sharma JP, Nagabhushanam Padala SR, Kushwaha J, Yadav SS.
Considerations to prevent intraoperative fluid spillage into the airway from a bronchogenic cyst during anesthesia: a case report.
A&A Practice 2022;16:e01625.
Updated: November 2022