(Esophageal lung)
Very rare (< 200 published cases). Abnormal communication, of congenital origin, between the esophagus and a bronchus, whether lobar or segmental (right side in 95 % of cases): in case of direct connection to a main bronchus, it is called esophageal lung. It is due to a disorder of embryogenesis between the 32nd and the 41th day of life. The origin is multifactorial with a possible genetic predisposition. The lung corresponding to the bronchus is either hypoplastic or consists in an extralobar sequestration. Vascularization can be systemic (aorta and inferior vena cava, portal or azygos vein) or pulmonary (intralobar sequestration) or mixed. Other malformations, especially esophageal ones, are often associated: esophageal atresia with or without fistula, VACTERL.
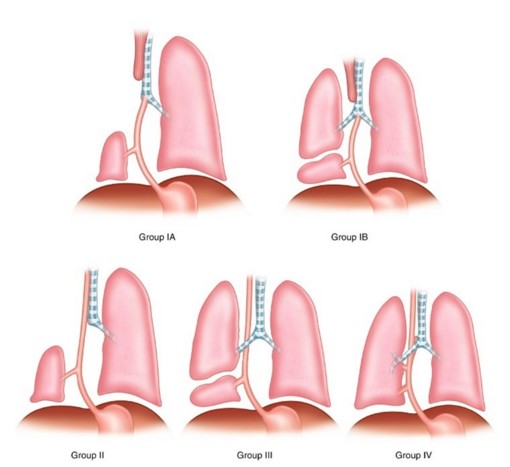
There are 4 different groups:
- I (16 %): associated with esophageal atresia with or without a tracheoesophageal fistula
* Ia: the whole lung originates from the bronchus coming from the esophagus or the stomach
* Ib: only part of the lung originates from the bronchus from the esophagus or the stomach
- II (33 %): one lung originates from the bronchus from the esophagus
- III (46 %): part of the lung (extralobar sequestration) originates from the bronchus from the esophagus or the stomach; vascularisation from the aorta or a hypoplastic branch of the pulmonary artery.
- IV (5 %): one section of the normal bronchial tree (right inferior (43 %) or left lobe (22 %) is communicating with the esophagus (inferior 2/3); the part of the lung coming from the bronchus has a systemic vascularization
Clinical presentation: neonatal onset or later, respiratory failure during the correction of an esophageal atresia, recurrent respiratory infections. The anomaly is sometines diagnosed late, during childhood (infections, persistent atelectasis, hemoptysis) or at adulthood (oblique pathway, presence of a ball valve effect ?)
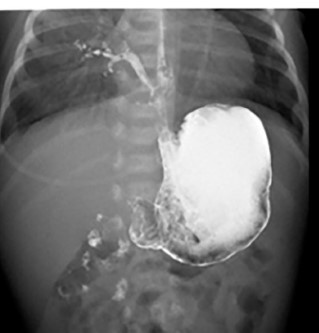
Diagnosis: RX, ultrasound, opacification, or esophageal endoscopy.
Treatment: resection of abnormal lung tissue or sequestrum. Sometimes, reinsertion of the bronchus on the trachea if the lung tissue is normal and if the diagnosis is early enough.
Anesthetic implications:
respiratory distress, thoracotomy (or - scopy) and one-lung ventilation in a newborn or infant; associated malformations.
In one reported case: ventilation of the healthy lung was achieved via the trachea and the remaining lung was ventilated separately through the intubated esophagus until the anastomosis of the esophageal bronchus to the trachea.
References :
- Srikanth MS, Ford EG, Phillip S, Mahour GH.
Communicating bronchopulmonary foregut malformations: classification and embryogenesis.
J Pediatr Surg 1992; 27: 732-6.
- Michel JL, Revillon Y, Salakos C, De Bloc J, Jan D, Beringer A, Scheinmann P.
Successful bronchotracheal reconstruction in esophageal bronchus: two case reports.
J Pediatr Surg 1997; 32:739-42.
- Peuch C, Malbezin S, Saizou C, Couloigner V, Elmaleh M, Nivoche Y, de Lagausie P, Laundenbach V.
Separate-lung ventilation strategy for reimplantation of esophageal bronchus.
Anesth Analg 2002; 95 : 333-5.
- Désir A, Ghaye B.
Congenital abnormalities of the intrathoracic airways.
Radiol Clin N Am 2009; 47: 203–25
- Sugandhi N, Sharma P, Agarwala S, Kabra SK, Gupta AK, Gupta DK.
Esophageal lung: presentation, management, and review of literature.
J Pediatr Surg 2011; 46: 1634-7.
- Trisno SL, Higano NS, Kechele D, Nasr T, Chung W, Zorn AM, Woods JC, Wells JM, Kingma PS.
Case report: Esophageal bronchus in a neonate, with image, histological, and molecular analysis.
Frontiers in Pediatrics 2021 ; 9 :707822.
- Patrao FM, Valdez AL, MD, Kanmanthreddy S, Gentry KR, Collins MJ.
Esophageal Bronchus—the hidden Link. A case report.
A&A Practice 2024;18:e01843
Updated: October 2024