(Erb or Erb-Duchenne paralysis)
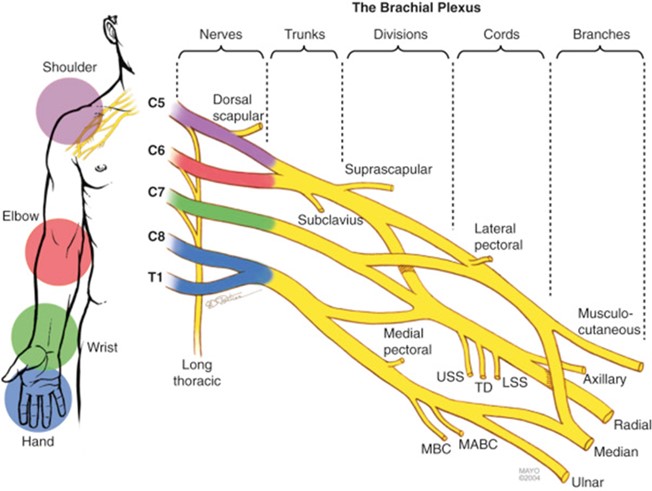
The overall incidence is between 0.42 and 2.9/1000 live births. By definition, neonatal brachial plexus paralysis is the weakness or flaccid paralysis of an upper limb diagnosed shortly after birth, and caused by a lesion of at least one cervical or thoracic nerve root (C5 to T1): it can be due to the stretching, rupture or avulsion (tearing from the spinal cord) of one or more nerve roots. This condition is often debilitating and can affect a child's overall development and quality of life. The clinical presentation can vary between transient weakness and global paresis, with the passive range of motion being greater than the active motion.
Possible causes are:
- shoulder dystocia at birth (excessive downward pulling after the head is delivered)
- injury either in utero or during descent into the pelvic canal (e.g., uterine abnormalities such as the bicornuate uterus)
- injury sustained at the time of expulsion
There is a strong association with an ipsilateral humeral fracture and clavicular fracture. A moderate association was observed with maternal diabetes, forceps or vacuum assisted delivery, fetal or neonatal asphyxia, macrosomia (greater than 4.5 kg), and a large for gestational age newborn.
The Narakas classification is used to classify the severity of the injury. The prognosis also depends on the type of nerve damage:
- neurapraxia: the myelin sheath is interrupted, resulting in a temporary conduction block; full function is usually restored within a few weeks
- axonomesis: lesion of the myelin sheath and axon but the perineurium and the epineurium are intact; some function is restored after a few months
- neurotmesis: complete rupture of the myelin, axon and supporting fibrous structures; frequent formation of a neuroma
- nerve avulsion: the root or roots have been torn from the spinal cord; no spontaneous recovery is possible and the repair is complex; risk of pseudomeningocele
Classification de Narakas
|
group |
name |
Affected roots |
signs |
|
I |
classic upper root paralysis (Erb's palsy) |
C5 or C6 |
absence of shoulder abduction, external rotation of the arm, elbow flexion, forearm supination |
|
II |
extensive superior root paralysis (Erb's palsy) |
C5 to C7 |
idem as I
|
|
III |
total paralysis without Claude Bernard-Horner syndrome |
C5 to T1 |
complete flaccid paralysis |
|
IV |
total paralysis with Claude Bernard-Horner syndrome |
C5 to T1 + sympathetic chain (sometimes the phrenic nerve is involved) |
complete flaccid paralysis + Claude Bernard-Horner syndrome (and homolateral diaphragm paralysis) |
Klumpke's palsy corresponds to the involvement of the C8 and T1 roots, and leads to paralysis of the hand.
Differential diagnosis:
- pseudoparesis following humeral or clavicular fracture, or local infection
- arthrogryposis
- neonatal neuromuscular pathology (spinal muscular atrophy, congenital myotonia etc.).
Surgical treatments: Groups I and II are associated with a higher rate of spontaneous resolution at 12 months (80 % and 60 %). Infants with total plexus injury (groups III and IV) showing no signs of recovery at 3 months require reconstructive microsurgery to explore and if possible repair the plexic us lesions and improve the prognosis: failure to restore biceps function at three months of age is generally considered as an indication for surgery before 6 to 9 months of age.
Two types of reconstruction:
- primary reconstruction: direct repair, neurolysis, nerve transplantation or nerve transfer. The "donor" nerves are taken either from the plexus (fascicles of the median or ulnar nerve, pectoral nerve) or a nearby (accessory spinal, intercostal) nerve. The sural nerve is rarely used.
- secondary reconstruction: joint capsulotomies, tendon transfers, soft tissue resection, osteotomies etc.
Anesthetic implications:
the disappearance of
References :
- Volpe KA, Snowden JM, Cheng YW, Caughey AB.
Risk factors for brachial plexus injury in a large cohort with shoulder dystocia.
Arch Gynecol Obstet 2016;294 : 925-9.
- Meena R, Doddamani RS, Sawarkar DP, Agrawal D.
Current management strategies in neonatal brachial plexus palsy.
J Peripher Nerve Surg 2021;5:1–7.
Updated: October 2022