(Opitz Trigonocephaly-like syndrome, Bohring-Opitz syndrome, Oberklaid-Danks syndrome, BOS)
Prevalence < 1/106. Mutation of the ASXL1 gene (20q11.21). Sporadic cases. Phenotype similar to the C syndrome.
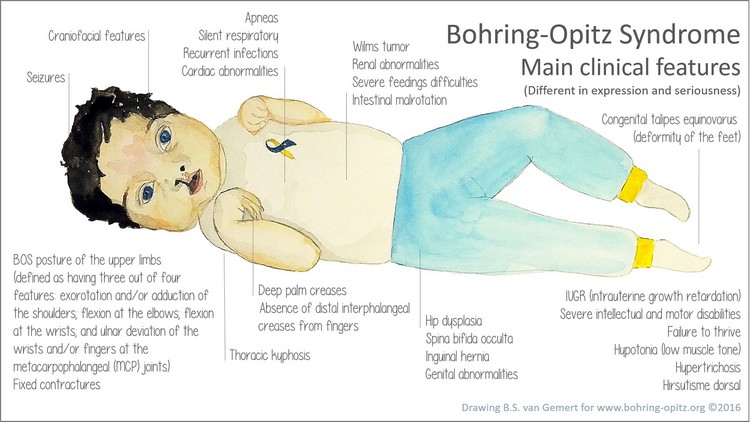
Clinical presentation:
- intrauterine growth retardation
- failure to thrive
- dysmorphism: prominent metopic ridge, naevus flammeus on the forehead, low frontal hairline with hirsutism, chubby cheeks, upslanting palpebral fissures, exophthalmos, hypertelorism, cleft lip and cleft palate, retrognathia and low-set ears
- elbow and wrist flexion, camptodactyly, ulnar deviation of the fingers, deep plantar creases.
- brisk episodes of bradycardia of unknown origin with a risk of sudden death; a cardiac malformation is sometimes associated (VSD, ASD, ventricular hypertrophy)
- feeding disorders with frequend vomiting of poorly determined origin: severe gastroesophageal reflux or cyclic vomiting
- risk of epilepsy
- sometimes sacral dimple and spina bifida occulta
- risk of nephroblastoma (Wilms Tumor)
Anesthetic implications:
short stature, risk of difficult intubation, difficult venous access, risk of aspiration (induction/recovery of anesthesia), epilepsy
References :
- Bohring A, Grétel G, Oudesluijs GG, Grange DK, Zampino G, Thierry P.
New cases of Bohring–Opitz syndrome, update, and critical review of the literature.
Am J Med Genet Part A 2006; 140A:1257–63
- Barry D, MacSweeney K, Barry G, O’Brien B.
Anaesthesia and Orphan diseases: Bohring- Opitz syndrome.
Eur J Anaesthesiol 2021; 38: 788-90
Updated: June 2021