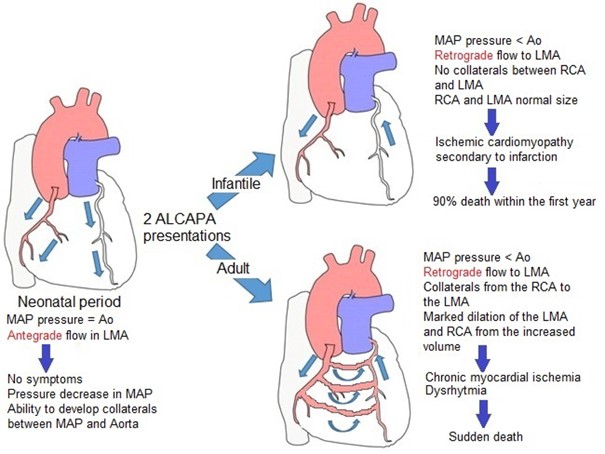
(ALCAPA acronym for Anomalous Left Coronary Artery arising from the Pulmonary Artery)
Very rare: 1/300,000 births. Anomaly of the origin of the left coronary artery: it arises from the pulmonary artery.
It is isolated in 95 % of cases but is associated with another malformation (ASD, VSD, coarctation of the aorta) in 5 % of cases.
In the majority of the cases, known as 'infantile-type ALCAPA', there are signs of ischemia of the left ventricle (dyspnea, sweating during meals, pallor) and heart failure (mitral regurgitation, dilated cardiomyopathy) as soon as the pressure in the pulmonary artery decreases i.e. within weeks (on average, 8 weeks) following birth or postoperatively following the correction of an associated cardiac malformation; 90 % mortality in the first year of life in the absence of surgical repair.
About 10 % cases, called 'adult-type ALCAPA', the whole myocardium gets progressively perfused from the dilated right coronary via developped collateral vessels: they are little (rhythm disorders, respiratory infections, delayed growth etc.) or not symptomatic and can survive to adulthood (risk of sudden death during exercice).
Anesthetic implications:
Avoid myocardial ischemia and coronary steal (the flow of the normal right coronary artery flows back to the PA via the left coronary artery): maintain a normal diastolic pressure and avoid any increase of the afterload of the LV (risk of an increased LV end-diastolic pressure). Avoid any decrease in the pulmonary resistance and pressions (hyperventilation) as it increases coronary steal phenomenon.
Diagnosis not to be missed in case of intraoperative cardiac arrest with signs of myocardial ischemia in infants. Sometimes the dilated left atrium (heart failure) compresses the left bronchus.
References :
- Sheinbaum RJ.
Cardiac arrest and resuscitation in a child with undetected anomalous left coronary artery.
Anesthesiology 1990; 72:1091-3.
- Kleinschmidt S, Grueness V, Molter G.
The Bland-White-Garland syndrome. Clinical picture and anaesthesiological management.
Paediatr Anaesth 1996; 6:65-8.
- Heidegger T, Waidelich E, Kreienbuehl G.
Anomalous origin of the left coronary artery: discovery during an ambulatory surgical procedure in a 3-month old, previously healthy infant.
Paediatr Anaesth 2001; 11:109-11
- Fahy CJ, Ing RJ, Kern FH, O’Hare B, Redmond JM, Jaggers J.
The anesthetic management and physiologic implications in infants with anomalous left coronary artery arising from the pulmonary artery.
J Cardiothor Vasc Anesth 2012; 26: 286-90.
- Serio P, Chiappa E, Fainardi V, Favilli S et al.
ALCAPA and massive pulmonary atelectasis : how a stent in the airway can be life-saving.
Int J Pediatr Otorhinolaryngol 2014; 78: 2015-7.
- Patra C, Singh NG, Manjunatha N, Bhtt A.
Anaesthetic management of infants posted for repair of anomalous origin of left coronary artery from pulmonary artery.
Indian J Anaesth 2017; 61: 676-8.
- Pena E, Nguyen ET, Merchant N, Dennie C.
ALCAPA syndrome
RadioGraphics 2009 ; 29 : 553-65.
- Bichali S, Giroux N, Benbrik N, Liet J-M.
Unexplained near-drowning can reveal ALCAPA in children.
Arch Pédiatr 2021 ; 28 : 252-4.
Updated: April 2021