Prevalence: 1/5000 births with a male preponderance; the risk of associated abnormalities is double in boys compared to girls.
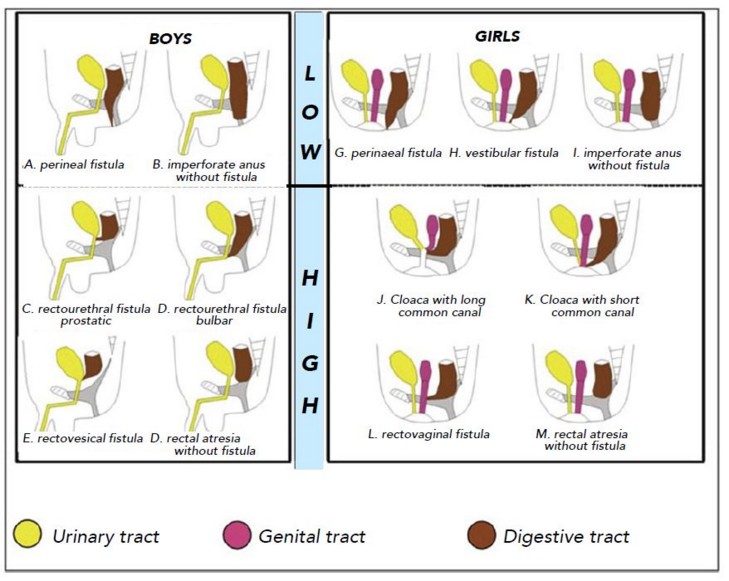
A distinction is made between high and low malformations because their embryological origin (time of gestation) and their surgical management are different.
The upper forms result from a disruption of the partitioning phase of the embryonic cloaca before the 8th week of gestation: the urogenital and digestive tracts remain connected (recto-urinary fistula in boys, recto-vaginal in girls). Some bone and musculo-nervous hypoplasia is associated.
The low forms occur after the partitioning of the cloaca: the malformation is limited to the anus (anteposition, stenosis, rectoperineal fistula) without communication with the urogenital system.
Table 1 presents the clinical classification and Table 2 the European radiological classification of the anorectal malformations:
.jpg)
The upper forms without fistula are particular: they affect both sexes equally and are frequently associated with trisomy 21; in addition, their functional prognosis is excellent because there is no sacral hypoplasia.
The anteposed anus is a normal anus located too close to the vulva from which it is only separated by a skin bridge. Sometimes the anteposed anus is joined to the vulva by a perineal groove (see this term).
The precise diagnosis of the malformation is established on a clinical and echographic examination of the perineum supplemented, if necessary, by a fistulography. The classic procubitus image taken at least 8 hours after birth to distinguish high and low forms according to the distance between the air in the rectal cul-de-sac and the projection of the puborectal strap is no longer used because there are too many false positives and negatives.
Anorectal malformations are generally the result of punctual defects in organogenesis but they can be part of polymalformative syndromes such as:
- VACTERL (Vertebral anomalies, Anal atresia, Cardiac defect, TracheoEsophageal fistula, Renal abnormalities, Limb abnormalities)
- the OEIS complex: omphalocele, bladder exstrophy, imperforate anus and spina bifida
- the MURCS association: Mullerian agenesis (uterovaginal aplasia), renal agenesis, cervical vertebrae abnormalities (Mayer-Rokitansky-Küster-Hauser syndrome type 2)
- the Baller-Gerold syndromes, cat's eye, caudal regression, Christian, Currarino, facio-auriculo-vertebral, Feingold, fetal alcoholism, Fraser, Ivemark, Johanson-Blizzard, Kabuki, Klippel-Feil, MIDAS (microphthalmia, aplasia of the dermis and sclerocornea), Okihiro, Smith-Lemli-Opitz, Pallister-Hall, Pallister-Killian, Rieger, Townes-Brocks, ulnar-mammary, Walker-Warburg (see these terms).
- chromosomal abnormalities: trisomy 13, 18 or 21, deletion 13q, deletion 22q11.2
This is why, in addition to digestive, renal and cardiac explorations, a radiological and echographic assessment of the lumbosacral spine must be carried out because sacrum and lumbar spinal cord (tethered cord, lipoma) abnormalities are often associated with.
Treatment:
- the perineal mucous groove is usually repaired between 6 and 12 monthsof age via a perineal approach,
- the anteposed anus is corrected only in case of functional disorders (constipation).
- in the other low forms, the surgeon performs, in the neonatal period, either a simple anoplasty in the gynecological position or a posterior sagittal anorectoplasty (in English PSARP, acronym of "Posterior Sagittal AnoRectoPlasty) in ventral decubitus.
- in the upper forms, a sigmoid discharge colostomy is performed 24 to 48 hours after birth while waiting for the definitive correction of the malformation when the child weighs more than 5 kg; this colostomy is closed during a third operation. In case of rectovesical fistula, abdominal surgery is performed in the supine position: a laparoscopic approach is possible for abdominal time. In other forms, a posterior sagittal anorectoplasty is currently performed in ventral decubitus. The rectum is approached through a median incision of the intergluteal groove, remaining perfectly on the midline. This approach has the advantage of avoiding damage to the nerve elements controlling the mechanisms of fecal continence. Two steps are performed by this approach: 1) the closure of the fistula between the terminal rectum and the urethra; 2) the pull-through of the rectum and its positioning in relation to the external sphincterian elements.
To perform a posterior sagittal anorectoplasty, the infant is positioned in the ventral decubitus position and its pelvis is raised to facilitate the surgical approach: it is therefore necessary to avoid compression of the chest and abdomen but also to protect the areas of skin compression (hips, upper part of the chest, face).
To avoid the development of anorectal stenosis, these children require, for several months, twice-daily calibrations using a Hegar dilators of suitable diameter. These sessions can be performed by the parents during a diaper change but short-term general anesthesia is required in case of stenosis, difficulties or fecaloma.
Anesthetic implications:
cardiac, renal and lumbosacral spine and cord echography; neonatal anesthesia and digestive occlusion (unless there is a large fistula). In the absence of involvement of the lumbosacral spine and cord, caudal or lumbar epidural block may be combined with general anesthesia for each of these procedures. In the newborn with associated severe malformations, the neonatal cure of low forms can be performed under spinal anesthesia alone if surgery is of short lasting.
References :
- Reding R.
Malformations anorectales. In Pathologie anorectale de l’enfant et de l’adolescent.
Reding R (ed). Médecine-Sciences Flammarion, Paris 2005, p 7-15.
- Sacrista S, Kern D, Fourcade O, Izard P, Galinier P, Samii K, Cathala B.
Spinal anaesthesia in a child with hypoplastic left heart syndrome.
Pediatr Anesth 2003; 13:253-6.
- Stafrace S, Lobo L, Augdal TA, avni FE, Bruno C, Damasio MB, Darge K et al.
Imaging of anorectal malformations: where are we now? Abdominal imaging task force of the European Society of Paediatric Radiology.
Pediatr Radiol 2022 ; 52 :1802-9.
Updated: August 2022