La prévalence de l'affection est d'environ 1/3.000 à 1/4.000 naissances vivantes, sans prédominance ethnique mais avec une légère prédominance masculine (3/2,5). Malformation congénitale caractérisée par une interruption de la continuité de l'œsophage entre sa portion distale qui est atrétique et sa portion proximale qui est dilatée et se projette entre la 2ème et la 4ème vertèbre thoracique. La fistule trachéo-œsophagienne est une variante d'atrésie de l'œsophage caractérisée par une communication anormale entre la trachée et l'œsophage qui peut se situer à n'importe quel niveau entre le cartilage cricoïde et la carène. Il existe une forme de fistule trachéo-œsophagienne non associée à une atrésie de l'œsophage que l'on désigne souvent sous le terme de fistule en H (H-type fistula en anglais).
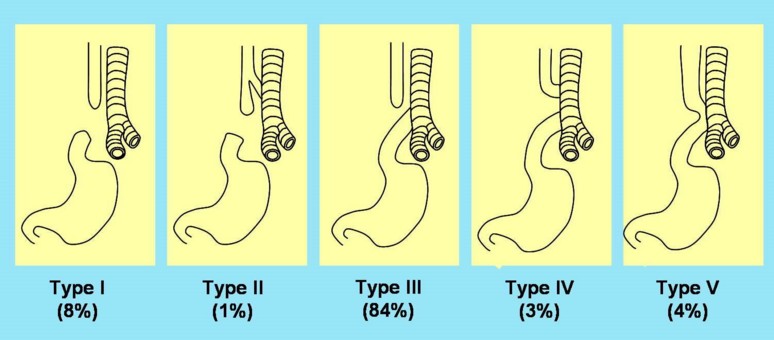
Il existe plusieurs classifications des atrésies œsophagiennes et fistules trachéobronchiques. La plus utilisée décrit 5 types de fréquence inégale :
- type I (ou A): atrésie de l'œsophage pure, sans communication avec la trachée (6-8 % des cas)
- type II (ou B) : atrésie de l'œsophage avec fistule entre le bout proximal et la trachée, l'extrémité distale de l'œsophage étant borgne (1 à 3 % des cas)
- type III (ou C) : atrésie de l'œsophage avec fistule entre le bout distal et la trachée, l'extrémité proximale de l'œsophage étant borgne : c'est la forme habituelle (84 % des cas) ;la fistule se situe habituellement 1 à 2 cm au-dessus de la carène, en situation postérieure, mais elle peut parfois siéger au niveau de la carène ou d’une bronche souche; ; la fistule s’abouche Á la partie postÕrieure de la trachÕe et se situe habituellement dans sa partie distale (43 %) ou 1 Á 2 cm au-dessus de la carÒne (33 %), mais elle peut parfois siÕger au niveau de la carÒne (17%) ou de la bronche souche droite (2 %);
- type IV (ou D) : atrésie de l'œsophage avec double fistule trachéale (bout proximal et bout distal) (3% des cas)
- type V (ou type E, ou fistule en H) : fistule entre la trachée et l'œsophage dont la continuité n'est pas interrompue mais est souvent sténotique (2,5 - 4 % des cas).
Certains auteurs rajoutent un type VI (ou F) dans lequel il existe seulement une sténose œsophagienne partielle, forme rare qui peut n'être découverte qu'à l'âge adulte. Les fréquences ont été calculées à partir d'une compilation des données provenant d'études de suivi à long terme d'enfants atteints par la malformation.
Il semble que la fréquence de la pathologie augmente légèrement avec l'âge maternel. Le diabète, l’alcool, une phénylcétonurie maternelle et le méthimazole sont des facteurs tératogènes possibles. Les facteurs génétiques ne semblent pas jouer un rôle important dans le développement de la malformation en dehors du syndrome d'Edwards (trisomie 18) et de cas particuliers bien identifiés qui ont permis de mettre en évidence le rôle probable de plusieurs gènes distincts:
- le syndrome de Feingold (ou syndrome oculo-digito-œsophago-duodénal) [MIM 164 280] de transmission dominante et associant en proportions diverses une microcéphalie, des malformations des membres, des atrésies œsophagienne et duodénale, un retard mental plus ou moins marqué ; des mutations des gènes MYCN ou miR-17-92 sont impliquées
- le syndrome AEG ou de Rogers [MIM 206 900] (acronyme en anglais de "Anophthalmia-Esophageal-Genital", c'est-à-dire "anophtalmie, atrésie de l'œsophage, malformations génitales"); mutations du gène SOX2
- le syndrome CHARGE (acronyme en anglais de "Coloboma, Heart defect, Atresia choanae, Retarded growth and development, Genital hypoplasia, Ear anomalies/deafness", c'est-à-dire "colobome, malformations cardiaques, atrésie choanale, retard de croissance et/ou retard mental, hypoplasie génitale, anomalies des oreilles et/ou surdité") [MIM 214 800] ; mutations du gène CHD7 dans 70% des cas
- l’anémie de Fanconi [MIM 227 650, 300 514, 227 645, 605 724, 603 467, 602 996] : l’atrésie de l’œsophage y est présente dans environ 15% des cas
- la dysostose mandibulofaciale de type Guion-Almeida [MIM 610 536] qui associe acrodysostose, microcéphalie, dysmorphie faciale et retard intellectuel ; mutations du gène EFTUD2
La cause la plus probable de la malformation est une élongation et une séparation incomplètes de la portion de l'intestin antérieur survenant entre la 4e et la 6e semaine de vie intra-utérine.
Les nouveau-nés atteints d'atrésie de l'œsophage sont souvent prématurés et hypotrophiques (poids de naissance < 1500 g dans 20 à 30% des cas). Dans la moitié des cas environ, la malformation est isolée (atrésies non syndromiques) ; dans les autres cas (atrésies syndromiques), il existe diverses malformations associées:
- malformations cardiaques isolées (25 %) : CIV, CIA, tétralogie de Fallot, canal atrioventriculaire, coarctation de l'aorte ;
- malformations complexes (13 %), en particulier dans le cadre d'une association VACTERL (anomalies vertébrales, anorectales, cardiovasculaires, trachéœsophagiennes, rénales, génito-urinaires et des membres) [MIM 192 350]; une forme rare de VATER est transmise de façon récessive ou liée à l’X et inclut une hydrocéphalie (VACTER –H) [MIM 276 950, 314 390]
- persistance d’une veine cave supérieure gauche.
- stÕnose trachÕale sous le niveau d’abouchement de la fistule.
Le risque de mortalité est d’environ 5,1 %% dans les pays développés : il est quasi nul chez le nouveau-né né à terme et sans anomalie associée mais augmente :
- s’il pèse moins de 1000g (x 8,6),
- si l’âge gestationnel est inférieur à 30 semaines
- en présence d’une malformation cardiaque majeure (x 6)
- en présence d’un syndrome (x 1,8 en cas de VACTERL, et x 3,9 en cas de trisomie 21).
- et, paradoxalement, en cas de diagnostic prÕnatal (formes plus souvent associÕes Á d’autres anomalies)
En cas de difficultÕs pour rÕaliser l’anastomose entre les deux extrÕmitÕs de l’oesophage, certains chirurgiens rÕalisent une approximation des cul-de-sacs Á l’aide de quelques sutures afin de favoriser la crÕation d’une fistule puis d’une anastomose spontanÕe entre ces deux lumiÒres (technique dite 'Suture Fistula').
Implications anesthésiques:
- intervention néonatale
- bilan malformatif y compris de quel c¶tÕ est la crosse de l’aorte (si Á droite : une thoracotomie gauche Õtait classiquement recommandÕe mais ce point est contestÕ) : Õchocardiographie, anus, morphologie
- anesthÕsie nÕonatale : glycÕmie, tempÕrature, TA, NIRS, SpO2 prÕ- et post-ductale
- thoracotomie (dÕcubitus latÕral) ou thoracoscopie (dÕcubitus quasi ventral) ?
- en cas de détresse respiratoire : attention, une gastrostomie peut aggraver les choses (fuite de la ventilation)
- induction en maintenant la respiration spontanée pour éviter la distension gastrique
- de nombreuses Õquipes rÕalisent une trachÕoscopie (souple ou rigide) en respiration spontanÕe avant l’intervention dans le but de localiser la fistule et d’exclure la prÕsence d’une seconde fistule, d’un diastÒme laryngÕ (2,5 %), d’une trachÕomalacie (85 % dont 30 % de formes sÕvÒres : > 80 % de collapsus expiratoire de la trachÕe); cet examen doit õtre complÕtÕ par une oesophagoscopie rigide si aucune fistule n’est observÕe lors de la trachÕoscopie afin d’exclure une atrÕsie de l’sophage sans fistule (type I) ou une perforation iatrogÒne du pharynx
- intubation : idéalement, de manière à occlure l’orifice trachéal de la fistule ; on peut cathéteriser la fistule avec une sonde de Fogarty pour faciliter la ventilation jusqu’à sa ligature. Cette procÕdure est trÒs utile en cas de fistule carinaire ou de stÕnose trachÕale serrÕe sous la fistule (on peut alors intuber avec une sonde de calibre normal au-dessus de la stÕnose.
- risque d’extubation accidentelle lors des manipulations intrabuccales pour placer une sonde gastrique transanastomotique
- patient en décubitus latéral et compression du poumon supérieur : risque d’hypoxémie ; la communication constante avec le chirurgien est importante
- il est recommandÕ de ne plus ligaturer la veine azygos pour Õviter la congestion veineuse autour du site anastomotique.
- post-opératoire : soit intubation durant 24-48h soit extubation en fin d’intervention (cathéter paravertébral ou péridural caudo-thoracique)
- en cas de distance trop importante entre les deux parties de l’sophage (¨ long-gap £) chirurgie diffÕrÕe : pose d’une gastrostomie, parfois d’une oesophago- ou pharyngo-stomie, pose de fils de traction sur les culs-de-sac oesophagiens (technique de Focker); parfois remplacement de l’sophage par une ilÕo-, gastro- ou coloplastie
- post-opératoire
- risque de fuite anastomotique ou de re-fistulisation précoce (5 %) avec médiastinite
- sténose anastomotique (20 %) nécessitant des séances de dilatation oesophagienne ou extraction en urgence d’un aliment bloqué: œsophage plein !
- risque de récidive (3 %)
- en cas de trachÕomalacie importante, une aortopexie ou mieux une trachÕopexie postÕrieure peut õtre rÕalisÕe
- reflux gastro-oesophagien
- hyperréactivité des voies aériennes : reflux, trachéomalacie
- rare : présence d’un diverticule de la paroi trachéale au niveau de l’abouchement de la fistule avec risque d’impaction de la sonde endotrachÕale et de difficultÕs de ventilation.
Références :
- Knottenbelt G, Costi D, Stephens P, Beringer R, Davidson A.
An audit of anesthetic management and complications of tracheo-esophageal fistula and esophageal atresia repair.
Pediatr Anesth 2012; 22: 268-74
- Arbell D, Golender J, Khalaileh A, Gross E.
Search for the azygos : a lesson learnt from a case with left superior vena cava, esophageal atresia and tracheo-esophageal fistula.
Pediatr Surg Int 209 ; 25 : 121-2
- Evans WN, Kogut K, Acherman RJ.
Preserving the azygos vein when repairing esophageal atresia and tracheoesophageal fistula accompanied by interrupted inferior vena cava.
Pediatr Surg Int 2014; 30: 345-7
- Diaz LK, Akpek EA, Dinavahi R, Andropoulos DB.
Tracheoesophagel fistula and associated congenital heart disease: implications for anesthetic management and survival.
Pediatr Anesth 2005; 15:862-9.
- Sapin E.
Perforations iatrogènes œsophagiennes chez le prématuré.
Arch Pédiatr 2003; 10:374-8.
- Bicakci U, Tander B, Ariturk E, Rizalar R, Ayyildiz SH, Bernay F.
The right-sided aortic arch in children with esophageal atresia and tracheo-esophageal fistula: a repair through the right thoracotomy.
Pediatr Surg Int 2009; 25:423-5.
- Krosnar S, Baxter A.
Thoracoscopic repair of esophageal atresia with tracheoesophageal fistula: anesthetic and intensive care management of a series of eight neonates.
Paediatr Anaesth 2005; 15:541-6.
- Tsao K, Lee H.
Extrapleural thoracoscopic repair of esophageal atresia with tracheoesophageal fistula.
Pediatr Surg Int 2005; 21:308-10.
- Deanovic D, Gerber AC, Dodge-Khatami A, Dillier CM, Meuli M, Weiss M.
Tracheoscopy assisted repair of tracheo-esophageal fistula (TARTEF): a 10-year experience.
Pediatr Anesth 2007; 17:557-62.
- Filston HC, Chitwood WR Jr, Schkolne B, Blackmon LR.
The Fogarty balloon catheter as an aid to management of the infant with esophageal atresia and tracheoesophageal fistula complicated by severe RDS or pneumonia.
J Pediatr Surg 1982; 17:149-51.
- Kovesi T, Rubin S.
Long-term complications of congenital esophageal atresia and/or tracheoesophageal fistula.
Chest 2004; 126:915-25.
- Dinner M, Ward R, Yun E.
Ventilation difficulty secondary to a tracheal diverticulum.
- Cheng AT, Gazali N.
Acquired tracheal diverticulum following repair of tracheo-oesophageal fistula : endoscopic management.
Int J Pediatr Otorhinolaryngol 2008; 72:1269-74.
- Mathew PJ, Ashok V, Malik MA.
Ventilation failure due to endotracheal tube migration into a tracheal pouch in a toddler with a repaired tracheoesophageal fistula: a case report.
A&A Practice, in press
- van der Zee DC, Lindeboom MYA, Tytgat SHA.
Error traps and culture of safety in esophageal atresia.
Sem Pediatr Surg 2019; 28: 139-42
- Dingemann C, Eaton S, Aksness G, Bagolan P et al.
ERNICA Consensus Conference on the management of patients with esophageal atresia and tracheoesophageal fistula: diagnostics, preoperative, operative, and postoperative management.
Eur J Pediatr Surg 2020;30:326-36.
- Fischer J, Balleisen J, Holski J, Cernaianu G et al.
Tracheoscopic findings and their impact on respiratory symptoms in children with oesophageal atresia.
Eur J Pediatr Surg 2020; 30: 371-7.
- Wolter NE, Kennedy AA, Michael J, Rutter MJ, Matava C, Honjo O, Chiu PL, Propst EJ.
Diagnosis and management of complete tracheal rings with concurrent tracheoesophageal fistula.
Int J Pediatr Otorhinolaryngol 2020 ; 133 :109971
- Kaufmann J, Laschat M, Schieren M, B—ckenholt K, Klein T, Wappler F.
Hypopharyngeal perforation mimicking esophageal atresia: a case report of an extremely low birth weight infant emphasizing the need for preoperative endoscopy.
A&A Practice 2021; 15: e1414
- Sfeir R, Rousseau V, Bonnard A, Gelas T, Aumar M et al.
Risk factors of early mortality and morbidity in esophageal atresia with distal tracheoesophageal fistula: a population-based cohort study.
J Pediatr 2021; 234:99-105.
- Obeida A, Magdy B, Taher H, Qinawy M, Elbarbary M.
Absent Azygos vein in a neonate with oesophageal atresia and tracheoesophageal fistula.
J Pediatr Surg Case Reports 2023 ; 90 : 102588
- Tan Tanny S, Newman SE, Safe M, Teague WJ.
Spontaneous anastomosis of esophageal atresia without esophageal stricture formation: A case report.
J Pediatr Surg Case Reports 2025; 115: 102972
Mise à jour octobre 2025